The Pharmacist’s Duty in Advancing Diabetes Care
Bill is a 55 year old male with type 2 diabetes diagnosed eight years ago. The diagnosis was shocking to him as he considered himself healthy and had no symptoms before the diagnosis. He has a family history of heart disease and his father died of heart attack at age 60. Bill’s BMI is 28, his blood pressure and HDL are controlled with medication and his diabetes was under control (A1c 6.9%) with metformin 2000 mg daily and glimepiride 8 mg daily for the last year. He has noticed symptoms of peripheral neuropathy and says the doctor is a little concerned about his kidneys. Today his A1c is 7.4% and Bill wonders why. He says he has not changed anything so why is the medicine not working like it should? He says the doctor may have to start him on insulin and that worries him.
 |
|
Sometimes we look back and wish we had done things differently and now it’s too late to reverse the damage. That happens to a lot of people with diabetes, maybe they don’t know they have it or they do and don’t control it, whether by conscious choice, or because they are unable or unwilling to get the treatments that are needed. Maybe they are uninformed and therefore not able to evaluate or make rational decisions on available remedies.
What can we do to be a part of the solution?
|
Therapeutic Inertia & the Progressive Nature of Type 2 Diabetes
Therapeutic inertia is defined as ‘failure to initiate or intensify therapy when appropriate to do so”. Numerous studies have verified this phenomenon and various reasons have been postulated for its existence. Our system of treating diabetes has been described as failure-based. Historically, we wait until something bad happens and react instead of proactively manipulating treatment regimens to slow progression and reduce complications.
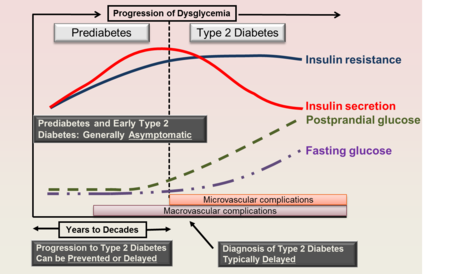
Type 2 diabetes is a progressive disease: years before type 2 diabetes is diagnosed, during the prediabetes state, the onset of insulin resistance results in an increased insulin secretion in order to keep blood glucose under control. Over time the pancreas is unable to keep up with insulin requirements and glucose levels rise to the level where diabetes is diagnosed. At that point about 50% of the beta cell functionality is lost. Increased cardiovascular risk occurs during the prediabetes stage. Maintaining tight control early in the disease process may help preserve beta cell function and reduce complications.
Addressing Therapeutic Inertia
Screening
Anyone with diabetes should be referred to a Diabetes Self-Management Education and Support Program (DSMES). Those at risk for diabetes should be referred to their healthcare provider and a National Diabetes Prevention Program (DPP).
Encourage monitoring
Patients with diabetes should be encouraged to use meaningful glucose monitoring over time to recognize changes in control that might indicate a need to adjust therapy. This can be done with home glucose monitoring or Continuous Glucose Monitoring (CGM), if qualified, and consistent A1c testing.
A1c testing is recommended at least every 6 months for patients who are stable and meeting treatment goals and every 3 months for those not meeting goals or undergoing therapy changes. Patients need to know their target A1c and their current A1c.
Are we looking at our patients' medication regimens with a critical eye?
 Right medicine, right dose, right time
Over time, even those individuals who are following all the lifestyle and medication guidance may experience challenges in diabetes management. Patients need to understand that challenges may occur and are a normal part of diabetes management. to know that and expect it. They also should be informed about medication options available to them.
Source: Ramlo-Halsted BA, Edelman SV. Prim Care. 1999;26:771-789
ADA guidelines state that a patient’s therapy should be reassessed and modified if needed every 3-6 months.
Patients now have the opportunity to receive medications that improve A1c while simultaneously addressing comorbid conditions, help with weight loss, and reduce risk of hypoglycemia Current guidelines recommend including an SGLT-2 inhibitor or a GLP-1 RA for people with or at high risk of for ASCVD. For patients with heart failure with reduced ejection fraction, an SGLT-2 inhibitor is recommended. For patients with established chronic kidney disease (CKD) an SGLT-2 inhibitor is recommended if possible. Interestingly, these recommendations stand regardless of the A1c level.
“The times they are a changing”
As in Bill’s case, the times are changing but there is reason for optimism. What advice would you give him?
Pharmacists have the obligation to inform patients about the best treatments available in a proactive manner. Newer treatments may not be an option because of cost or some other reason but at least we have done what we could to keep that patient informed. Becoming a DSMES provider or a Diabetes Care and Education Specialist (DCES) is a great way to further the care you provide. The Montana Diabetes Program can help you accomplish this goal!
Better options are out there for diabetes patients with diabetes. Let’s help them get what they need!
James Bennett, RPh, CDCES, BCGP
Bozeman MT
Resources:
ADA Standards of Care App
Diabetes Risk Test available on ADA website
American Diabetes Association Standards of Care 2021
Please share with any and all colleagues, encourage them to Click to subscribe!
|