
Honoring Black History
Black History Month first began as Negro History Week. It was created in 1926 by Carter G. Woodson, known as the “Father of Black History.” This historian aimed to encourage “people of all ethnic and social backgrounds to discuss the Black experience”. By the late 1960s, the civil-rights movement led to a growing awareness of Black identity. Negro History Week was celebrated by mayors in cities across the country. Eventually, this celebration evolved into Black History Month on many college campuses. In 1976, President Gerald Ford officially recognized Black History Month. He urged Americans to “seize the opportunity to honor the too often neglected accomplishments of Black Americans in every area of endeavor throughout our history”. In 1986, the U.S. Congress passed "National Black History Month" into law and people began to observe it formally. The law aimed to make all Americans "aware of this struggle for freedom and equal opportunity".
Sage asks that we take this month to honor all Black people from all periods of United States history and show respect and recognition for the hard work and sacrifices that have been made.
Minneapolis is hosting several Black History Month Events, many of which can be joined remotely: City of Minneapolis Black History Month Events https://www.minneapolis.org/calendar/holidays/black-history-month/
|

Paying tribute to our Country’s Black Public Health Leaders
Black History Month was initially used as a way of teaching students and young people about Black and African-Americans’ contributions. Such stories had been largely forgotten and were a neglected part of the national narrative. Black History Month is now seen as a celebration of those who've impacted our country and world with their activism and achievements. The month-long spotlight is an opportunity to engage with Black histories, to go beyond discussions of racism and slavery, and to highlight Black leaders and accomplishments.
Dr. Donna M. Christensen was the first woman to represent the U.S. Virgin Islands and the first female medical doctor to serve in Congress. She worked to address social determinants of health and tackle HIV/AIDS threats both domestically and internationally. She made it known that in medicine, “…you always find that there are a lot of social and other issues that impact the health of your patients.” Dr. Christensen was born in Teaneck, New Jersey. Her mother was from New York and her father, who served in the U.S. Army during World War II, returned to his native Virgin Islands with his young family after earning a law degree from Columbia University. Dr. Christensen’s interest in health began after she read a United Negro College Fund booklet encouraging young minorities to go into medicine.
William Carter Jenkins was an American public health researcher and academic. Jenkins was among the first cadre of African Americans recruited to the United States Public Health Service Commissioned Corps in the 1960s. He worked as a statistician and is best known for trying to halt the Tuskegee syphilis experiment in 1969. The Tuskegee Study of Untreated Syphilis in the Negro Male involved hundreds of black men who were told they were being treated for “bad blood,” a local term used to describe several ailments, including syphilis, anemia, and fatigue. The men did not receive proper treatment, and many died from untreated syphilis, despite the discover of penicillin (the treatment drug of choice) three decades before the study ended. Jenkins spent his career fighting racism in the U.S. healthcare system, working for the Centers for Disease Control and Prevention (CDC) during the early days of the AIDS crisis, and overseeing the government benefits program for survivors of the Tuskegee Syphilis Study.
Henrietta Lacks was an African American woman who died in 1951 at the age of 31 of an aggressive cervical cancer. Samples of Ms. Lacks cancerous cells were taken without her knowledge or consent and shared widely for research purposes. Ms. Lack’s cells turned out to have an extraordinary capacity to survive and reproduce, making them ideal for biological research. Her immortal cells, known as HeLa cells, have been involved in key scientific discoveries in the fields of cancer, immunology, and infectious diseases. None of the biotechnology companies that profited from HeLa cells asked for her family’s consent, nor did they pay for the use of her cells, though they used her name publicly, gave her medical records to the media, and published her cells’ genome online (which has since been removed). One of the most recent applications for use of HeLa cells has been in research for vaccines against COVID-19. The Lacks family and scientists are working together to establish stronger rules to govern the use of specimens.
Kizzmekia Corbett, PhD, is an African American National Institutes of Health scientist praised by top infectious disease experts for her role in developing the COVID-19 vaccine. Dr. Corbett received a PhD in microbiology and immunology from the University of North Carolina at Chapel Hill. Her early research involved studying the spike proteins on the surface of coronaviruses. Dr. Corbett’s team utilized previous knowledge of coronaviruses to tackle the COVID-19 virus. Throughout the politicized pandemic, Dr. Corbett has called for the public to practice good hygiene and worked to build vaccine trust among Black Americans.
Sherman A. James is an African American epidemiologist and health researcher. Dr. James is known for his concept “John Henryism,” which attributes the premature deaths of African Americans to prolonged exposure to the stress, discrimination, and racism. The name of his hypothesis is based on the American folk hero, John Henry. John Henry was purported to have raced against a steam-powered rock-drilling machine, and he won, but died from the effort. In commenting on why Black men live shorter lives than all other Americans, Dr. James stated, “It’s the striving to make something of themselves …to live their lives with dignity and purpose and to be successful against extraordinary circumstances. They’re trying to make a way out of no way. It’s the Black American story.”
Please join us in our efforts to reduce health disparities, advance health equity & during the month of February and all year celebrate the richness and accomplishments of our ancestors.
For more information, visit: Black History Public Health
|

Breast Cancer Champions Fight for Health Equity for African American Women
Since 2020, the Breast Cancer Champions Project has brought together Minnesota’s female community leaders to act as peer educators to share the message that breast cancer screening is very important to the women in our communities, and to assist these women in accessing breast cancer screening services and resources in environments that help them feel safe and supportive. This collaborative project has come to life though the strong partnerships between the Minnesota Department of Health, the Breast Cancer Education Association, the University of Minnesota and Sisters Standing Up to Breast Cancer.
A total of 14 champions have been trained, and currently 9 are active. Of these 9 champions, four are from immigrant African communities, and five are African American. The Champions reach out to women in a variety of ways: through churches, hair salons, local food shelves, and social media. Champions share information about breast cancer, the disparities experienced by African American and immigrant African communities and offer breast cancer screening appointments to women in these focus communities. Through this important intervention women are both educated about their greater breast cancer risk and also navigated through the cancer screening process.
Since the start of this project, Champions have reached over 2300 women and have referred 448 women for screening mammograms. In 2021 alone, the Champions participated in 24 screening events, (21 of the 24 with on-site mammography), with 228 women having completed their mammograms at these events.
The Champions truly do make a difference to the women in their communities by offering support, guidance, and advocacy that can lead to changes in health disparities and inequities around breast cancer.
|
Breast and Cervical Cancer in MN’s African American Women
MN is one of the nation’s healthiest states, yet it experiences significant health disparities and inequities. The burden of breast and cervical cancer is not equally distributed by race and ethnicity.
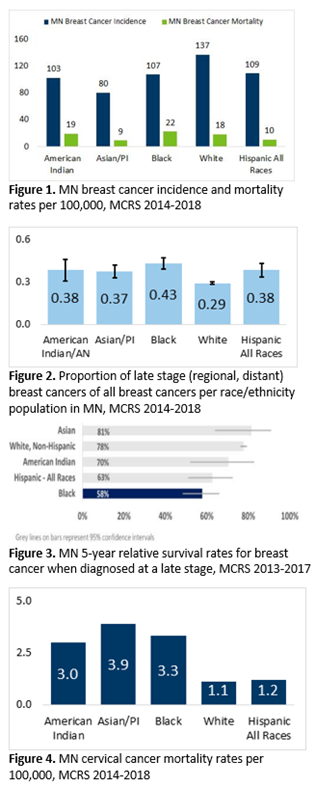
Breast cancer has been and remains one of the leading causes of death in African American women in Minnesota. Minnesota’s African American women have a 22% higher mortality rate than white women (Figure 1). This is despite African American women having a lower overall incidence of breast cancer (Figure 1) and only slightly lower screening rate (72.0% vs. 76.3%).1 African American women are also diagnosed at a later-stage than white women (43% vs 29%), Figure 2, and have a significantly lower 5-year relative survival rate than whites (58% vs. 78%) as observed in Figure 3.
Cervical cancer outcomes also show disparities for Minnesota’s African American women. African American women are 3 times more likely to die from cervical cancer compared to white women (Figure 4).
Several factors may account for racial differences in breast and cervical cancer stage of diagnosis and mortality including socioeconomic factors, access to screening and timely treatment, and genetics. Sage is committed to prioritizing screening for MN’s African American women and connecting them to timely treatment following a diagnosis.
Despite African American women only being 6.2% of Minnesota’s population, they represent 11% of Sage’s patient base. Furthermore, nearly 10% of breast cancers diagnosed in Minnesota’s African American women are detected through the Sage Program. Sage sees it as critical to implement culturally appropriate interventions in Minnesota’s communities to improve African American women's breast and cervical cancer screening participation by minimizing barriers and engaging entire African American communities – including residents, religious leaders, health care providers and other breast and cervical cancer stakeholders. Sage looks forward to strengthening partnerships with MDH programs, Minnesota Cancer Alliance participants, Minnesota’s health care plans and systems, and non-profit and community organizations that work toward decreasing disparities and increasing health equity among our African American communities.
-
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2014-2020

SagePlus can support African American women to improve their Heart Health
African Americans face an increased burden of health risks related to cardiovascular disease. In 2018, African Americans were 30% more likely to die from heart disease than non-Hispanic whites. Although African American adults are 40 percent more likely to have high blood pressure, they are less likely than non-Hispanic whites to have their blood pressure under control. African American adults are 60 percent more likely than non-Hispanic white adults to be diagnosed with diabetes by a physician. This data shows us how important it is to have a program available that can help address these issues. That program is SagePlus!!
For more information on African American heart health, visit:
Office of Minority Health: Heart Disease and African Americans
SagePlus Solutions – Screening and Intervention
SagePlus is a heart health screening program for women enrolled in the Sage breast and cervical cancer screening program. This program gives women the opportunity to address their risks for cardiovascular disease. SagePlus participants are screened for obesity, smoking, diabetes, high cholesterol, and high blood pressure (hypertension). Participants then receive education about their personal risk factors. It is very important to “know your numbers”, especially when it comes to diabetes and high blood pressure.
Next, women can decide to participate in Healthy Behavior Support Services. These services may include 1-on-1 visits with nutritionists, pharmacists, diabetes educators or smoking cessation counselors. Other participants may choose to join group nutrition classes, physical activity classes, weight loss support groups, or at-home blood pressure monitoring programs. SagePlus patient navigators and health coaches are there to support and encourage women on their journey to better heart health.
SagePlus Solutions – Recruitment and Outreach
SagePlus staff make special efforts to recruit and connect with women in the African American community. We partner with Hennepin Health clinics on targeted outreach efforts in the metro area. Because African American women may face challenges or delays in screening and treatment for heart disease and stroke, it is very important to do our best to reach SagePlus eligible women.
SagePlus staff also have planned screening events with dedicated appointments for African American women to join our program. Benita Robinson, SagePlus patient navigator, is onsite at clinics during screening events to answer questions and support women to complete paperwork. Reports are also run to monitor enrolled women to ensure interventions are completed in a timely manner. Open communication and close partnerships with clinic staff are key to SagePlus reaching women who could benefit the most from improved heart health.
|
|



