|
November 2019
Paperless certifications and digital solutions discussed at national conference
Vital records professionals along with their federal, corporate, and public health partners met at the 2019 NAPHSIS Identity and Security Conference in Washington, D.C., earlier this month. NAPHSIS, the National Association for Public Health Statistics and Information Systems, convened the conference to explore a future with biometrics, paperless certifications, mobile access, and user controlled data sharing.
Because technology, customers’ needs, and the demand for real-time information are driving change, the Office of Vital Records (OVR) sent six Minnesotans to the event. OVR sought proposals from county staff to explain how they would share and apply what they learned from the experience with their colleagues. Selected were Barbara Olson, Regional Manager for the Hennepin County Government Center and Ridgedale Service Centers Division; Julie Hanson, Scott County Property and Customer Service Manager; and Carol Schmaltz, Otter Tail County Recorder. MR&C IT supervisor Troy Stein, OVR Security and Records Supervisor, Brenda Shinaul, and State Registrar, Molly Crawford completed the group.
In addition to demonstrations for mobile driver’s licenses and hearing about New York City’s biometric authentication for birth registrars, funeral directors, and medical certifiers, Jeremy Grant, from the Better Identity Coalition, discussed the coalition’s policy recommendations and five common-sense initiatives that are practical to implement and have meaningful impact:
- Prioritize the development of next-generation remote identity proofing and verification systems.
- Change the way America uses Social Security numbers.
- Promote and prioritize strong authentication.
- Pursue international coordination and standardization of identity systems.
- Educate consumers and businesses about better identity solutions.
Read the full report Better Identity in America: A Blueprint for Policymakers (PDF). Also discussed at the event were global impacts and the need for all of us to have an identity—a legal identity.
Watch Vital Records News for more information and training about identity and serving customers in new ways.
The author of this article works with the Diabetes Unit in the Child & Family Health Division at the Minnesota Department of Health.
Asian women in Minnesota have the greatest prevalence of gestational diabetes mellitus (GDM) compared to women in other racial/ethnic groups, which is consistent with national data1. However, the Asian racial/ethnic category includes women who have vastly different cultural practices and dietary habits. Minnesota is home to the largest Hmong population in the United States. Few studies have examined how the prevalence and risk of GDM differs between Asian subgroups, and very sparse, if any, research exists describing the prevalence of GDM among Hmong women. In these analyses, we sought to examine the prevalence and relative risk for GDM among Asian women, broken down by Asian subgroup, to better understand the differences in GDM prevalence and risk among Asian women.
Using 2016-2017 data from the birth certificate, we examined the prevalence and relative risk of gestational diabetes among Asian women who reside in Minnesota and gave birth to a live, singleton infant in Minnesota. We used a chi-square test to determine if the prevalence of GDM differed by Asian subgroup. Additionally, we calculated the crude and adjusted risk ratios (aRRs) and 95% confidence intervals (CI) of gestational diabetes for all Asian women combined and for the following Asian subgroups, as compared to non-Hispanic White women: Asian Indian, Chinese, Filipino, Korean, Vietnamese, Cambodian, Hmong, Laotian, and Other Asian. Risk ratios were adjusted for maternal age, insurance type, maternal education level, nativity (U.S.-born or born outside the U.S.), and parity.
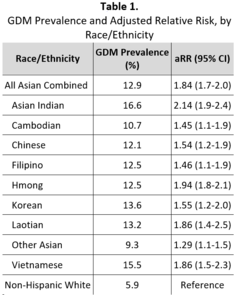
Overall, 12.9% of Asian women in Minnesota who gave birth to a singleton infant had gestational diabetes. The prevalence of gestational diabetes differed by Asian subgroup (p-value <0.0001), with Other Asian women having the lowest prevalence (9.3%) and Asian Indian women having the highest prevalence (16.6%) among Asian women (Table 1). After taking into account maternal age, insurance type, maternal education level, nativity (U.S.-born or born outside the U.S.), and parity, the risk of gestational diabetes for all Asian women combined was 84% greater than that for non-Hispanic White women (aRR = 1.84, 95% CI 1.7-2.0). Women in all Asian subgroups had a higher risk of GDM than did non-Hispanic White women. Among Asian women, Asian Indian (aRR = 2.14, 95% CI 1.9-2.4) and Hmong (aRR = 1.94, 95% CI 1.8-2.1) women had the greatest risk of GDM; Other Asian (aRR = 1.29, 95% CI 1.1-1.5), Cambodian (aRR = 1.45, 95% CI 1.1-1.9), and Filipino (aRR = 1.46, 95% CI 1.1-1.9) women had the lowest risk of GDM among Asian women.
In conclusion, the risk of GDM among Asian women varies within Asian subgroups, but all of the subgroups had higher risk of GDM when compared to non-Hispanic White women. Certain subgroups, especially Asian Indian and Hmong women, were twice as likely to have GDM, as compared to non-Hispanic White women. Women of Asian descent have a higher prevalence of GDM as compared to women in other racial/ethnic groups. However, most studies examining race/ethnicity and gestational diabetes aggregate Asian women into one racial/ethnic category. This study illustrates that aggregating all Asian women into one racial/ethnic category may mask differences in relative risk for gestational diabetes among women in different Asian subgroups; understanding these differences may help guide prevention efforts by taking into account specific cultural practices and dietary habits. Rates for GDM should be presented with the “Asian” racial category disaggregated into Asian subgroups whenever possible to better illustrate the health risks and outcomes of Asian women.
1Deputy NP, Kim SY, Conrey EJ, Bullard KM. Prevalence and Changes in Preexisting Diabetes and Gestational Diabetes Among Women Who Had a Live Birth — United States, 2012–2016. MMWR Morb Mortal Wkly Rep 2018;67:1201–1207. DOI: http://dx.doi.org/10.15585/mmwr.mm6743a2external icon.
Our thanks to Regina Marino, MPH for submitting this article. Regina is a Council of State and Territorial Epidemiologists (CSTE) Applied Epidemiology Fellow with the Diabetes Unit in the Child & Family Health Division at the Minnesota Department of Health. This study/report was supported in part by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists (CSTE) and funded by the Centers for Disease Control and Prevention (CDC) Cooperative Agreement Number 1 NU38OT000297-01-00.
|
|

