|
February 2018
Partnership between Surveillance and Vital Records Data
Influenza surveillance in Minnesota uses multiple surveillance systems to assess influenza activity levels. Long-term care facilities (LTCFs) and schools report outbreaks of influenza in their facilities, multiple outpatient clinics provide numbers of patients presenting with Influenza-like illness (ILI), and clinical laboratories throughout the state provide data on influenza testing and percent positivity. Hospitalized individuals with laboratory-confirmed influenza and individuals who have died from influenza and/or complications related to influenza are also reportable to the Minnesota Department of Health (MDH).
Influenza-associated deaths can be difficult to measure, but Minnesota relies on partnerships with hospitals, LTCFs, medical examiner’s offices, and Minnesota’s Office of Vital Records (OVR). OVR staff provide surveillance staff at MDH with a daily report of all death certificates filed with influenza listed as a cause of death (COD). Hospitals and LTCFs report individuals who have died as inpatients or as LTCF residents and medical examiners provide specimens which are tested for a number of infectious pathogens (UNEX program) at MDH.
The partnership between OVR and surveillance staff at MDH has greatly improved the ability to track influenza-associated deaths in the state. Individuals who pass away at home, even shortly after a hospital or LTCF discharge, can be very difficult to identify with standard surveillance methods; death certificate data improves our ability to track these deaths. OVR staff query the Minnesota Registration & Certification system (MR&C) daily to provide surveillance staff with real-time data for individuals with influenza listed as a COD who may have been otherwise unreported.
The influenza surveillance staff also use data provided by OVR to determine the number of individuals that die following a hospitalization for influenza. Surveillance staff match influenza-associated hospitalizations with annual death certificate data from OVR to ascertain influenza-associated deaths that may have been missed by other reporting methods.
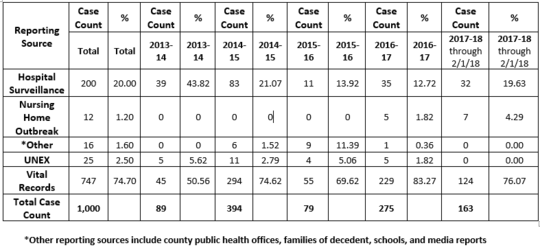
Through the partnership with OVR, influenza surveillance staff are able to collect death certificate data for influenza-associated deaths to assess other co-infections and high-risk conditions. These data allow us to better characterize trends and risk factors involved with influenza-associated deaths. Of the 1,000 influenza-associated deaths reported to MDH since October 1 of 2013, 708 (70.80%) have influenza listed as a COD, and only 14 (1.40%) individuals did not have death certificate data and/or a death certificate filed in Minnesota. In summary, 71% of reported influenza-associated deaths can be identified by the daily death certificate database (MR&C) query alone.
Below are data on influenza-associated deaths in Minnesota. ‘Reporting source’ refers to the source that reported the individual first. Many cases are reported by multiple sources. Influenza seasons span October 1 through May 31 of the following calendar year. This table illustrates how integral OVR data are to influenza surveillance staff. Overall, surveillance staff receive nearly 75% of influenza-associated death reports from OVR data, through a combination of the daily queries and matching death certificate data with influenza hospitalization data, as described above. Without this partnership, the burden of influenza-associated mortality would be drastically underestimated.
OVR
thanks Melissa McMahon, MPH, Senior Epidemiologist in the
Vaccine-Preventable Disease Surveillance Section at the Minnesota Department of
Health for contributing this article.
The Minnesota Department of Health (MDH) is moving all technical applications, like Minnesota Registration and Certification (MR&C), to Amazon Web Services (AWS), a cloud-based platform for storing and accessing data over the internet. This move brings three main benefits:
Saves money
Just as warehouses once stored enormous amounts of paper data, data centers now store electronic data. With more state business conducted online, the need for more space – and the cost associated with that space – has risen considerably. Cloud computing provides a cost-effective storage alternative. MDH pays only for the space it needs at any given time, and not for space it may or may not need at some point in the future.
Enhances security
MDH applications will be located in a “virtual private cloud” within AWS. This means that the data and official records maintained by MDH is isolated from other data stored in the cloud. AWS also provides MDH with resource monitoring, application security inspections, data encryption, identity and access management and protection from hackers.
Positions MDH for the future
AWS helps MDH fulfill its strategic goals by using modern and affordable technology to deliver services and programs to Minnesotans. It ensures that data and applications stay protected and supported, making disaster recovery quicker and easier. It also allows MDH more flexibility in responding to emerging public health threats.
The normal schedule of MR&C updates and improvements is on hold while migration work is underway. The Office of Vital Records (OVR) hopes that MR&C will be on the cloud by the end of June 2018.
Watch for more information in the coming months.
February is American
Hearth Month, a federally
designated event and reminder to focus on our heart health. It is also an ideal
time to examine how vital records is part of the conversation—especially birth
records. Birth registration requires reporting abnormal conditions and
congenital anomalies—including those that involve the heart.
The list of congenital anomalies on the birth record includes
cyanotic congenital heart disease. Cyanotic newborns look bluish or purplish
because the tissues just below the skin are not getting enough oxygen. Cyanotic
congenital heart disease is not one single disease or defect; the data item,
when checked, indicates that one or more conditions that cause cyanosis are
present. See page 42 of the CDC’s Guide
to Completing the Facility Worksheets for the Certificate of Live Birth and
Report of Fetal Death for a list of keywords and abbreviations. Record Cyanotic Congenital Heart Disease on the
birth record when any one of the following heart defects are present:
- Transposition
of the great arteries/ great vessels – this means the heart’s anatomy is
opposite of what is normal. The reversed structure changes the way blood
circulates through the body, causing a serious shortage of oxygen in blood
flowing from the heart.
- Tetralogy
of Fallot – indicates four heart abnormalities: a hole between the lower
chambers of the heart, an obstruction from the heart to the lungs, the large
artery that takes blood to the body (aorta) lies over the hole in the lower
chambers and the muscle surrounding the lower right chamber is thicker than
normal.
- Pulmonary
atresia & Tricuspid atresia – the valve controlling the blood flow from
the heart to the lungs (pulmonary atresia) or between the upper and lower
chambers of the heart (tricuspid atresia) is not present at birth.
- Truncus
arteriosus – one large artery instead of two separate ones to carry blood
from the heart to the lungs and body.
- Hypoplastic left heart syndrome – the left side
of the heart does not form correctly.
- Total/partial anomalous pulmonary venous return
with or without obstruction – the veins bringing blood back from the lungs do
not connect to the left atrium of the heart.
- Interrupted aortic arch/coarctation of the aorta
– the aorta is not completely developed.
Minnesota
has around 69,000 births each year. Fewer than 50 Minnesota birth records in each of the last
five years had the cyanotic congenital heart disease data item checked. While
these birth defects are not common, this birth record data seems underreported
when compared to the Minnesota Birth Defects Information System (BDIS). BDIS
compiles information about 45 conditions, including congenital heart defects,
diagnosed within the first year of life.
Birth registrars should familiarize
themselves with the list above. “Cyanotic congenital heart defects” is a category of defects; patient medical
records identify the specific defect and not the category label. Do not check
‘Other anomalies’ on the birth record and specify one of the defects above.
In most cases, babies born with cyanotic congenital heart
disease require surgery to repair the heart. This may mean transfer of the
newborn to a Neonatal Intensive Care Unit (NICU) – perhaps in another hospital.
Birth registrars must make extra efforts to follow up and accurately report the
health information when a newborn transfers to a NICU.
For more information:
-
Heart
Disease in Minnesota, another MDH website, has information about adult
heart disease — how common it is, disparities in heart disease rates, and the
economic costs of heart disease.
|


