|
On April 15, the Centers for Disease Control, National
Center for Health Statistics awarded funding to the Office of Vital Records (OVR)
for the Minnesota Paper Cut Project—a two-year effort to improve the timeliness
and quality of death registration. The award provides an operational framework and
assigns a high priority to increasing electronic death registrations through the
Minnesota Registration and Certification (MR&C) System.
Despite a long
history of electronic death registration since 1997, and recent successes in
improving death registration, OVR has not achieved full participation among
physician communities in using MR&C. This project provides the traction OVR
needs to change the death registration culture in Minnesota.
Together with partners, federal programs, and state staff,
OVR will use a multi-phased approach to assure that the infrastructure is in
place to support and sustain improved performance. The goals of the Paper Cut
Project are:
- Receive at least 80% of mortality records
electronically through MR&C
- Transmit death information collected through
MR&C to the National Center for Health Statistics within 10 days of the
date of death for at least 80% of deaths
- Share data about deaths related to
state-specified causes of deaths (Influenza, Methicillin-resistant
Staphylococcus aureus (MRSA), and Methicillin-Susceptible Staphylococcus aureus
(MSSA)), with MDH State Epidemiologists within one day of the cause of death being filed.
Ingrained paper processes waste
valuable time and consume limited resources because of redundant activities to
provide cause of death information. Statutory requirements for final
disposition authorization can be completely met and death registration can be
completely accomplished through MR&C. Paper complicates, competes with, and
prevents full use of the MR&C System.
The Paper Cut Project comes at a time when others see the
need for death registration improvement and are sensitive to the burden that
paper registrations outside of MR&C place on all partners. In February, the
Ramsey County Chief Medical Examiner, Dr. Michael McGee, established a no-paper
policy for cremation authorizations; his office is using MR&C to approve
requests for cremation. The move has had a cascading effect among clinics and
hospitals in the 16-county jurisdiction. In March, OVR staff recruited 116 new
physician users, nearly triple the number from the same time last year.
The Paper Cut Project does not require new laws or rules.
Within the current legal framework, OVR can focus resources on MR&C
enhancements and specifically on increasing physician use of MR&C. OVR will
continue to support new users of MR&C, one record and one physician at a
time, while expanding to a facilities-wide approach. In addition, Paper Cut
Project funding will:
- Create a new OVR call center and help desk to
support partners in the vital records system
- Expand training efforts for new and existing
MR&C users
- Enable a death record to be started with the cause
of death information (as opposed to the funeral home starting the death record).
OVR welcomes quality improvement efforts initiated by
external partners and will support them as part of the effort to eliminate
paper and unnecessary processes. “Precious resources are pushed to the limit
when business practices perpetuate paper when a fully functional electronic
death registration system exists,” said Molly Crawford, State Registrar. “Having
a solid foundation in place to support the push for online use and inviting
change will be important. Breaking the improvements into phases beginning
with the OVR framework will assure a strong infrastructure to support the
change and that resources are allocated appropriately to meet our partners’
needs and industry demands as the project progresses.”
OVR Finalizes 2015 Data Reporting to NCHS
The National Center for Health Statistics (NCHS) contracts
with 57 states and jurisdictions to collect birth, death and fetal death data. NCHS
standards for data quality require states to review data that may be unlikely,
incorrect, or inconsistent. All quality issues must be resolved according to
NCHS standards to close out a data year.
The Office of Vital Records (OVR) works with birth
registrars, physicians, and funeral directors to resolve any outstanding data
issues. Finalized data is then submitted to NCHS to meet the reporting deadlines.
The National Vital Statistics
Reports are a result of this effort.
In 2015, there were 69,095 birth records filed in Minnesota.
OVR, after working with birth registrars to correct
or verify data highlighted by NCHS for review, submitted final
2015 birth record data to NCHS before the March 1, 2016 deadline.
Death records must also meet NCHS data quality standards. 42,711
death records were filed in Minnesota for the 2015 reporting year. OVR staff
worked with funeral directors, physicians, and medical examiners to verify and
correct data quality issues that NCHS flagged, and met the May 1, 2016
reporting deadline.
NCHS also has data quality standards for fetal death reports.
Data items flagged for review by NCHS were reviewed with birth registrars or
medical examiners. In 2015, there were 390 fetal death reports filed in
Minnesota; finalized fetal death report data was submitted to NCHS to meet the May
1, 2016 deadline.
Each year, you, our partners in vital records, collect the
data needed to file vital events in Minnesota; in 2015, 112,194 birth, death
and fetal death report records were filed using the Minnesota Registration
& Certification System (MR&C).
We in OVR thank our partners in vital records sincerely for
their continued service, commitment and dedication to provide accurate and
timely records. One record at a time, our work informs public health and
improves lives.
OVR to examine self-reported birth data with health equity
lens
Advancing health equity is an essential goal for the Minnesota Department of Health (MDH) and initiatives to engage communities in program work is a priority for MDH. For these reasons and the rising trend of ‘unknown’ responses to data elements collected for birth records, the Office of Vital Records (OVR) launched a project to increase the completeness of birth record data. The Beginnings and Beyond Engagement (BABE) project specifically aims to improve self-reported data from mothers because a “health in all policies” approach to public health relies on complete and reliable vital records data.
BABE looks at the birth registration process and its critical impact beyond the beginning of a newborn’s life. The project looks beyond ‘going through the motions to collect data’, good or bad, and beyond simply reporting data to National Center for Health Statistics (NCHS), but starting to improve it. For OVR, BABE is an opportunity to engage facilities and data sources in new thoughtful and purposeful ways to improve processes and encourage data sources to provide complete and reliable data.
Over the next few months, OVR will examine hospital birth data, gather information about data collection and birth registration operations, and compare practices with outcomes. Staff from OVR will reach out to selected facilities and others to invite participation in the project and targeted improvement discussions and activities.
Education, race, ethnicity and cigarette use before and during pregnancy are four important data elements reported by mothers at the time of their child’s birth. For the last three years, in Minnesota, responses of ‘unknown’ for these data elements have trended upward.
Typically, the woman who gives birth completes the Mother’s worksheet for naming your baby and creating a birth record on paper as part of the birth registration process. The worksheet contains data fields for reporting education, race, ethnicity and cigarette use before and during pregnancy along with other items needed to complete the birth record.
The information supplied by the mother along with the health data collected during birth registration become elements of the birth record. When de-identified birth record data is shared with the National Center for Health Statistics, it becomes part of our nation’s official vital statistics. Public health professionals use vital records data and statistics to identify and monitor health problems, risk factors and disease patterns, and assess the impact of interventions.
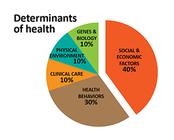
The four data items that OVR is examining contribute to an understanding of health inequities within Minnesota. Mother’s cigarette use (a behavioral factor) and her education level (a socio-economic factor) are considered high risk factors and are reviewed by MDH and local public health programs to identify resources for, and intervention needs of, mothers and newborns. The pie chart shows the significance that social and economic factors and health behaviors have on population determinants of health.
 |
|
Further, this information along with race and ethnicity are
important data that factor into the determinants of health. In fact, mother’s
race and ethnicity as reported on her child’s birth record is often used as her
child’s race and ethnicity. Birthplace is also an important data element used
in geocoding and assessing the health of communities such as the County Health Rankings &
Roadmaps tool which provides a useful visual display of data about health
outcomes.
|
|

