|
Quick Links: Tools for Infection Control in Health Care Settings | Emerging Infectious Diseases (EDI) Journal | EDI Podcasts
Jump to: Increase in invasive group A strep infections | C. auris
Increase in invasive group A strep infections
The CDC is looking into an increase in invasive group A strep (iGAS) infections among children in the United States. iGAS infections include necrotizing fasciitis and streptococcal toxic shock syndrome.
Current recommendations for health care providers include:
- Offer prompt vaccination against influenza and varicella to all eligible persons who are not up to date.
- Consider iGAS as a possible cause of severe illness, including in children and adults with concomitant viral respiratory infections. Illness due to iGAS in persons with known viral infections may manifest as persistent or worsening symptoms following initial improvement.
- Educate patients, especially those at increased risk, on signs and symptoms of iGAS requiring urgent medical attention especially necrotizing fasciitis, cellulitis, and toxic shock syndrome.
- Obtain culture for suspected iGAS infections, including blood, wound, and pleural fluid cultures, as clinically indicated.
- Follow clinical practice guidelines for diagnosis and treatment of GAS pharyngitis.
- Be mindful of potential alternative agents for treating confirmed GAS pharyngitis in children due to the shortage of amoxicillin suspension.
- Notify appropriate local or state public health departments as soon as possible about unusually aggressive or severe iGAS cases affecting children younger than 18 years of age or clusters of iGAS infections in persons of any age.
- Ask laboratories to hold iGAS isolates or send them to the state public health laboratory for temporary storage.
Amoxicillin Shortage: There is a national shortage of the liquid antibiotic (amoxicillin suspension) most often prescribed to children to treat group A strep infections. The shortage is anticipated to last several months.
Clinicians: View the American Academy of Pediatrics guidance for alternative therapies during the shortage.
Candida auris in Michigan
C. auris
Candida auris is a yeast that may colonize on the skin and other body sites, especially in hospitalized patients or long-term care facility residents. Patients colonized with C. auris may carry the organism without signs or symptoms, often for prolonged periods of time. Patients colonized with C. auris can go on to develop serious illness or invasive infections. C. auris is often multidrug-resistant which makes infections difficult to treat. C. auris can spread from colonized or infected patients to the hands and clothes of health care providers or to medical equipment and surfaces in health care environments, which may contribute to the spread of C. auris among patients in health care facilities. Therefore, preventing the spread of C. auris is a both a public health and health care priority.
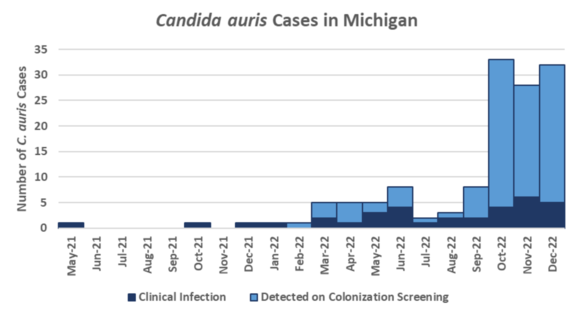
Surveillance and Epidemiology
The first case of C. auris in Michigan was identified in May 2021. Detections of C. auris increased significantly in 2022 and likely represents an emerging threat to patient safety. As of January 1, 2023, Michigan has detected 134 cases (see figure below). Most cases have been detected via colonization screening, which is often conducted as a result of exposure assessments that occur in response to new cases. Most C. auris cases have had multiple health care exposures across the continuum of care with 99% having had acute care hospital exposure 90 days prior to detection, 66% with a long-term acute care hospital (LTACH) stay, and 20% having previously resided in a skilled nursing facility (SNF). Other common factors identified among C. auris cases include presence of indwelling medical devices (e.g. 73% with recent mechanical ventilation), chronic or surgical wounds (67%), and prior history of multidrug-resistant organisms (MDROs).
 Of 21 C. auris clinical isolates with antifungal susceptibility testing, 95% were resistant to fluconazole, none were resistant to polyenes, and 19% resistant to echinocandins, compared with 88%, 34% and 3% from isolates tested nationally by CDC (Antifungal Susceptibility Testing and Interpretation).
Healthcare facilities are critical partners to controlling the spread of C. auris and should be familiar with how to detect C. auris, implementing infection prevention recommendations in response to cases, and assuring strong communication when transferring patients with a C. auris history.
Laboratory Detection of C. auris
Health care facilities are encouraged to develop a plan to detect patients with C. auris in their facility. Both the Michigan Department of Health and Human Services (MDHHS) Surveillance for Healthcare-Associated and Resistant Pathogens (SHARP) Unit and Bureau of Laboratories (BOL) are happy to assist facilities with developing a plan based on their current epidemiology and risk level for C. auris transmission.
Clinical Specimen Surveillance
Species-level identification for all yeast isolates from sterile sites is recommended. However, laboratories who have been speciating yeasts from non-sterile sites of high-risk patients have been instrumental in finding some of the early C. auris cases in Michigan. Laboratories should conduct species-level identification for yeast isolates when:
-
C. auris has been identified in the health care facility.
- A patient has a history of health care stay outside the US in the past 12 months.
- And considered for high-risk patient populations such as patients presenting from LTACH, ventilator-capable SNFs, ICUs, or rehabilitation facilities, particularly if they have risk factors for auris such as mechanical ventilation or tracheostomy, chronic wounds, or a history of MDROs.
Colonization Screening for High-Risk Patients
Health care facilities admitting patients at high-risk for C. auris should conduct colonization screening upon admission to the facility. Health care facilities are encouraged to identify laboratory resources to conduct colonization screening through in-house testing, commercial or reference laboratories. The MDHHS SHARP unit can also provide assistance for colonization screening to conduct point prevalence surveys and outbreak testing through our Regional Laboratory. The MDHHS BOL is currently working on developing capacity to conduct screening by Spring 2023.
Infection Prevention and Control
Health care facilities, across the continuum of care, should:
- Take steps to identify patients with auris infection or colonization.
- Be prepared to implement setting-appropriate infection prevention precautions, including the use of disinfect products effective against auris (see the EPA List P).
- Collaborate with local and state public health agencies on recommended IPC practices and colonization screening to detect asymptomatic auris carriage.
Transfers/Discharges Between Health Care Facilities
Per routine procedures for patients infected with MDROs, clear transfer communication is required to ensure appropriate precautions are taken when C. auris patients are moving facilities. Do include communication of lab results that are pending and/or finalized after the patient has been transferred.
Receiving health care facilities should take note of a patient’s C. auris status and be prepared to implement setting-appropriate precautions for C. auris patients, as they would for other MDROs. Facilities that care for patients with other MDROs or Clostridioides difficile are also capable of caring for patients with C. auris.
Facilities that would like to discuss caring for patients with C. auris may contact the Surveillance for Healthcare-Associated and Resistance Pathogens (SHARP) Unit at (517) 335-8165 or MDHHS-SHARP@michigan.gov.
|