Pediatric Syndromic Surveillance for COVID-19
Ali Bianco, MPH, Fatema Mamou, MPH, and Bethany Reimink, MPH
Throughout the COVID-19 pandemic, syndromic surveillance has been a valuable tool in providing near real-time data on COVID-19 related visits to Emergency Departments (EDs) and Urgent Care Centers (UCs). Data is currently obtained from 216 participating facilities across the state of Michigan (139 Emergency Department, 77 Urgent Care). Data fields collected for each visit include basic patient demographic information (age, sex, ZIP code), facility information, chief complaint. Most data streams also include discharge diagnosis.
Of note, due to the nature of categorizing chief complaint data, these visits do not represent all potential visits for COVID-19 and may include a limited number of non-COVID-19 illness complaints (e.g., from other respiratory viruses such as respiratory syncytial virus (RSV)). However, the data can be used to describe trends in illness presentations over time. Additionally, recent changes in healthcare seeking behavior, including increasing use of telemedicine and recommendations to limit ED visits to severe illness, as well as changes in ED triage practices and alternative COVID-19 testing sites are impacting ED and UC visits in Michigan. These changes affect the numbers of people and their reasons for seeking care in the ED and UC settings.
As a part of the Michigan Department of Health and Human Services (MDHHS) routine COVID-19 syndromic surveillance, visits are queried for different syndromic indicators of COVID-19, including pneumonia, mentions of coronavirus, COVID-19 discharge diagnosis codes, and chief complaints of self-reported symptoms that meet the CDC case definition of Coronavirus-Like Illness (CLI) - fever accompanied by cough and/or shortness of breath/difficulty breathing.
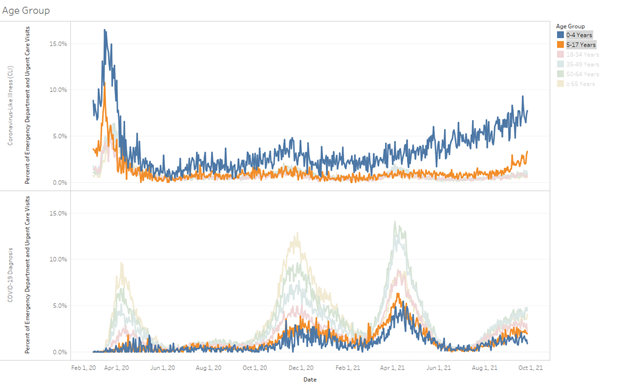
Syndromic surveillance for COVID-19 among children and adolescents has been especially important over the past few months as increasing rates of pediatric illness and hospitalization have been reported across the country. The following charts show the proportion of ED and Urgent Care visits in Michigan between March 1, 2020 and September 26, 2021 that had CLI (top chart) or a COVID-19 diagnosis (bottom chart), stratified by age. The 0-4 (blue) and 5-17 (orange) year-old age groups have been highlighted. While higher proportions of CLI have been seen in children throughout the pandemic, actual COVID-19 diagnoses among them have stayed relatively low compared to other age groups until late Summer 2021. The percent of COVID-19 diagnoses in children during late Summer and early Fall 2021 is higher compared to the same time period in 2020 and to-date has been continuing to increase.
In addition to COVID-19, syndromic surveillance has also been utilized to look for trends in Multisystem Inflammatory Syndrome in Children (MIS-C). MIS-C is a potentially serious condition in children and adolescents under the age of 21 years where multiple organ systems become inflamed. Many children with MIS-C are found to have been infected with or exposed to COVID-19 prior to developing MIS-C. By searching for visits with symptoms and discharge diagnosis codes that are common among MIS-C patients, MDHHS can better understand the burden of this syndrome and predict when and where there might be potential spikes in reported cases. Although MIS-C guidance is available to all MI healthcare providers, anticipated increases in cases may better direct targeted education.
For more information, visit the MDHHS COVID-19 Syndromic Surveillance webpage.
Title
|


