|
Tiffany Henderson, MPH - Regional Epidemiology Unit Manager - Michigan Department of Health and Human Services (MDHHS)
Influenza
has made its presence known this year, with the virus making state and national
headlines and closing down multiple schools in Michigan as well as across the
country. A recent study indicates that
in addition to droplets, the influenza virus may be spread through aerosols and
another study provides evidence of a significant association between flu and
subsequent heart attacks. As of the week ending January 20, 2018, Michigan, along
with 48 other states and Puerto Rico, reported widespread influenza activity. Various
data streams are used to conduct influenza surveillance in Michigan, including
the Michigan Disease Surveillance System (MDSS), the Michigan Syndromic
Surveillance System (MSSS), sentinel physician and laboratory surveillance, and
the Influenza Hospitalization Surveillance Project (IHSP). According to sentinel physician surveillance
data from ILINet for the week ending January 20, approximately 3.6% of
statewide visits were due to influenza-like-illness (ILI), which is above the
regional baseline of 1.8%. This is the seventh consecutive week this indicator
has been above the baseline. Laboratory surveillance from the MDHHS Bureau of
Laboratories indicates that the predominant circulating influenza strain is influenza
A H3N2, followed by influenza B. In addition, the IHSP uses data on hospitalizations
due to severe ILI through active surveillance and chart review of lab-confirmed
cases for Clinton, Eaton, Ingham, Genesee, and Washtenaw counties. Since October
1, there have been a total of 535 influenza-related hospitalizations reported
in the catchment area for this influenza season. As of January 29, 2018, no
pediatric influenza-associated deaths have been confirmed by MDHHS, but
nationally, 37 pediatric influenza-associated deaths have been reported.
In
addition to routine reviews and analyses of MDSS and MSSS data, Regional
Epidemiologists review the MSSS during the flu season for indicators of ILI. The
MSSS is a voluntary system that collects chief complaint and basic patient
information from visits to Emergency Departments (EDs) and Urgent Care Centers and
categorizes those complaints into one of ten syndromic categories. Increases in
constitutional visits (e.g., fever, chills, malaise, fatigue) correlate with
other influenza and ILI surveillance indicators. Special reports that look
specifically at ILI visits (i.e., chief complaint of self-reported flu or chief
complaint meets the CDC case definition for ILI (fever accompanied by sore
throat and/or cough)) are conducted during the influenza season for the state
and each region (statewide graph below). The majority of the public health
preparedness regions continue to experience increasing proportions of visits
due to ILI and constitutional illness.
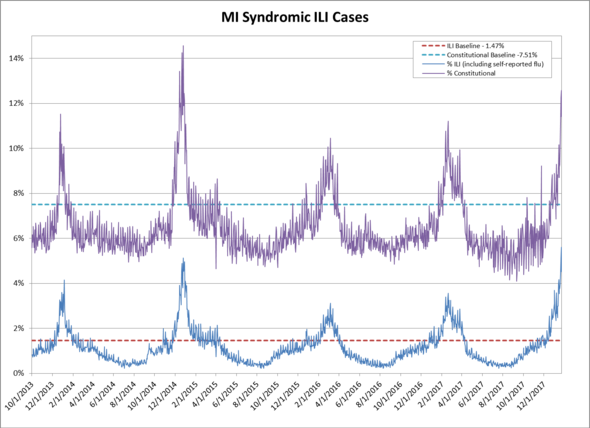
The following graph shows the proportion of ILI and constitutional
complaints reported to the MSSS from October 1, 2013 – January 29, 2018. For
comparison, the graph includes ILI and constitutional baselines, which represent
the average proportion of ILI or constitutional complaints for the past four
mild influenza seasons (2007-2008, 2008-2009, 2010-2011, 2011-2012).
 ILI activity is also measured through reports
of congregate setting outbreaks to public health from schools, long-term
care/assisted living facilities, and other facility types. For the current
influenza season, 122 respiratory viral outbreaks have been reported, including
outbreaks in the corrections system. During recent outbreaks, impacted prison
facilities implemented daily symptom monitoring, visit restrictions, unit
quarantine, case isolation, and environmental cleaning. Control measure discussions also included the
logistics and implications of restricting visitors and altering prisoner
transfers. In addition, due to the
nature of the congregate setting and potential for underlying risk factors in
this population, chemoprophylaxis was recommended. There have been concerns
about obtaining an adequate Tamiflu supply to meet the demand. Although there
is not an overall Tamiflu shortage at this time, local supplies can be quickly
exhausted during outbreaks in large congregate settings. Additional Tamiflu can be ordered, but may
delay timely administration and so advanced planning is paramount.
MDHHS
continues to review surveillance streams for influenza and ILI. It is not too
late to get vaccinated. The Centers for
Disease Control and Prevention is predicting that influenza activity will
continue for several more weeks and even healthy people can become seriously
ill from the flu. With influenza and
other viruses circulating, it is also important to practice good hand hygiene
to protect yourself and those around you. For more information, including the
most recent MI Flu Focus, please visit www.michigan.gov/flu
Guidelines for Influenza and Respiratory
Virus Outbreaks in Long-Term Care Facilities Document
| 

