|

Alaska Department of Health and Social Services Weekly COVID-19 and Influenza Update April 24 – April 30, 2022
Key Findings
- COVID-19 transmission remained widespread in most parts of Alaska during the week of April 24–April 30, 2022, with evidence for increasing cases in some areas but decreases elsewhere.
- Influenza transmission increased during April after declining from a previous peak in late December 2021.
- Other respiratory viruses are circulating in addition to SARS-CoV-2 and influenza virus.
COVID-19
COVID-19 Case Trends
- COVID-19 transmission continues to occur widely throughout much of Alaska, with no clear upwards or downwards statewide trajectory. Cases and hospitalizations remain far below the peak of the Omicron wave.
- 1,445 cases were reported in Alaskans the week of April 24–April 30, which is an 8% increase compared to the previous week.
- The number of newly detected COVID-19 cases increased last week compared to the previous week in all five of the largest boroughs (Municipality of Anchorage, Matanuska-Susitna Borough, Fairbanks North Star Borough, Kenai Peninsula Borough, and City and Borough of Juneau). But overall, there have not been clear upward or downward trajectories in these communities over the past two months.
- The intensity of COVID-19 transmission varies between communities outside the largest boroughs. Trajectories are mixed, with COVID-19 cases declining in some boroughs and census areas but increasing in others. The number of new cases has begun to decline in some communities in southeast Alaska, while it may be still increasing in others. Some communities, especially in western Alaska, continue to experience large outbreaks relative to their population size.
- The Omicron variant accounts for effectively all SARS-CoV-2 circulating in Alaska. The BA.2 lineage (a sub-type of Omicron) has become dominant. Visit Alaska’s SARS-CoV-2 Genomics Dashboard to learn more.
- To learn more about COVID-19 cases, hospitalizations, and deaths due to COVID-19 in Alaska, visit the Cases Dashboard or the monthly report. The cases dashboard includes demographic information on cases and the monthly report includes demographic information on hospitalizations and deaths.
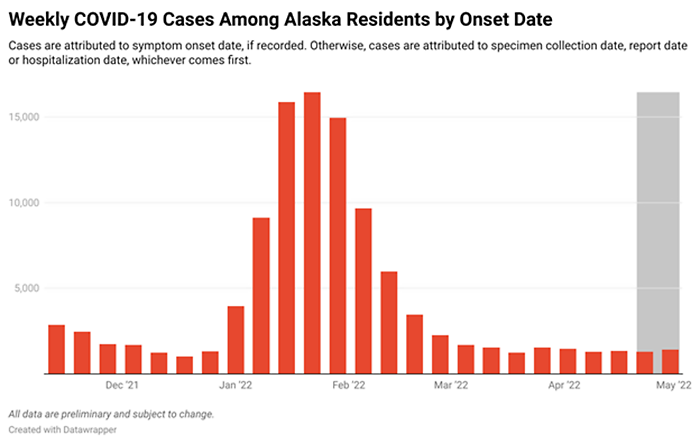
COVID-19 cases among Alaska residents by week of onset date.
Click here to sort data
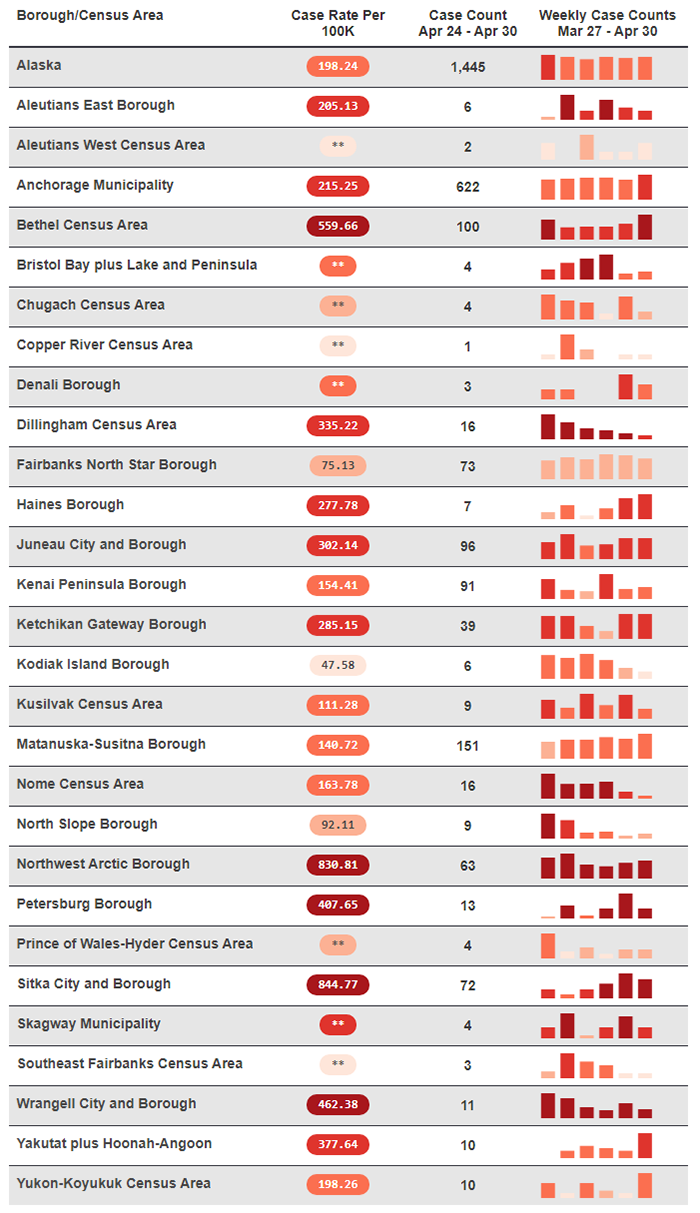
*Rates based on <20 observations are statistically unreliable and should be used with caution.
**Rates based on <6 observations are not reported.
Community case rates are based on case report date.
COVID-19 and Hospital Capacity
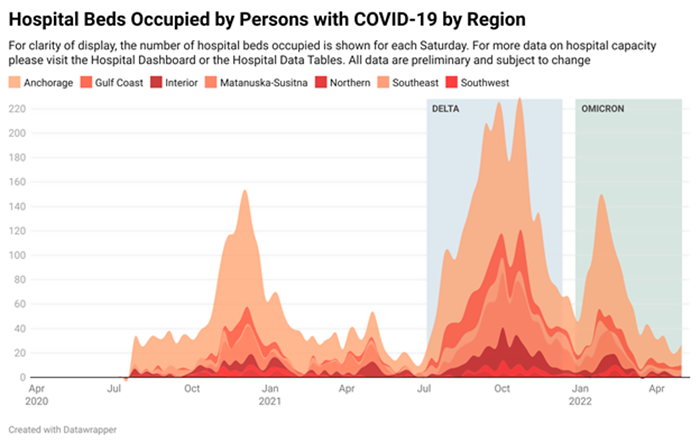
- Some regions continue to experience capacity limitations because of large numbers of patients overall (not necessarily with COVID-19 or other respiratory viruses) or due to staffing issues. However, overall, the state has returned to a more normal level of referral capacity for higher-level and specialty care.
- Patient Care Strategies for Scare Resource Situations are currently not being utilized by any facility in Alaska. However, the Crisis Care Committee continues to meet to monitor the situation and remains available to assist facilities and DHSS should the need arise.
- As of May 4, 2022, there were 33 persons with COVID-19 in Alaska hospitals, accounting for 2.6% of all hospitalized persons. Visit the Hospital Dashboard for more data.
COVID-19 and Vaccination
- 72.0% of Alaska residents aged ≥5 years have received at least one dose of a COVID-19 vaccine. Among those who completed the primary vaccine series, 51.2% of Alaska residents ≥18 years have received their booster. Learn more about COVID-19 vaccination coverage in Alaska on the Vaccine Dashboard. Learn more about COVID-19 vaccines.
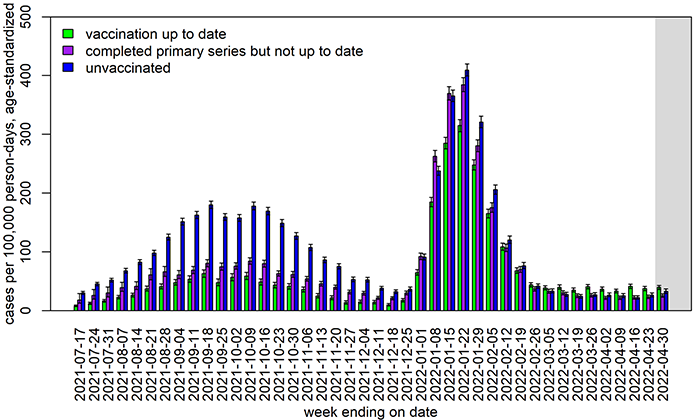
- Vaccines help protect against infection and against severe disease, especially when a person is up to date on vaccinations. During the 4-week period from March 27, 2022–April 23, 2022, the number of documented hospitalizations due to COVID-19 was too small to reliably calculate the relative differences in incidence rates by vaccination status. The age-adjusted incidence of COVID-19 hospitalizations was the highest in unvaccinated Alaskans and lowest in Alaskans up to date on COVID-19 vaccination. These estimates are lagged by one week to partially account for the time it takes to document hospitalizations. (See the monthly report for more data and analysis through January.)
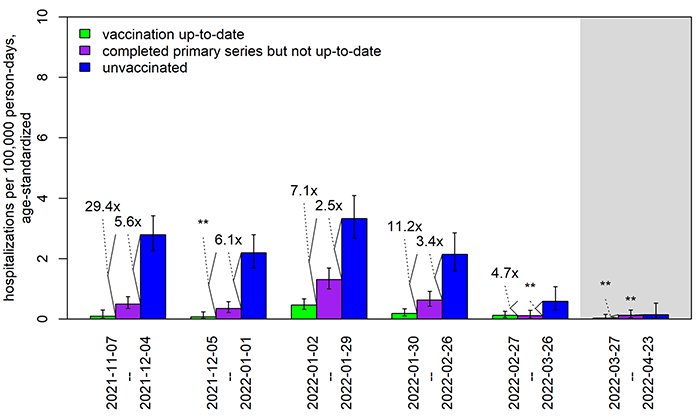
In order to more easily identify changes over time, the definition of “up to date” as of January 8, 2022, was applied to data from all time points. The absolute rates of hospitalization especially in the most recent 4-week period highlighted in grey are likely underestimates because of COVID-19 hospitalizations that have not yet been documented. **Especially when rates are very low, the estimates of fold-differences between rates may be imprecise. Fold-differences are not calculated if one of the rates is based on <6 cases.
- Among Alaska residents aged ≥5 years from January 16, 2021–April 30, 2022, 75,227 cases were documented in persons who had completed the primary series and were considered fully vaccinated. Among those vaccine-breakthrough cases, 544 hospitalizations and 198 deaths due to COVID-19 have been recorded. During that time, 101,039 cases have been documented in unvaccinated Alaskans aged ≥5 years, leading to 1,870 hospitalizations and 675 deaths. All data are preliminary and subject to change.
- During the Omicron wave, the incidence of COVID-19 cases in vaccinated persons has become more similar to the incidence in unvaccinated persons. This trend likely reflects multiple factors which may include: immunity wanes over time, cases in vaccinated persons may be more likely to be detected than cases in unvaccinated persons, and there may be increased infection-induced immunity especially among unvaccinated persons.
In order to more easily identify changes over time, the definition of “up to date” as of January 8, 2022 was applied to data from all time points. Some COVID-19 cases with specimen collection in the immediate past week (indicated by the grey box) may have not yet been reported or counted.
Influenza (“Flu”)
- Reported influenza cases began increasing in Alaska in mid-December but declined during January and remained relatively flat through February and March. Cases began increasing in April, with the number of reported cases the week of April 24–April 30 greater than the number reported the previous week.
- Right now, most influenza in Alaska is caused by influenza A.
- 24% of Alaskans aged ≥10 years have been vaccinated against seasonal influenza. It is not too late to get vaccinated against influenza.
- Learn more in the weekly Alaska Influenza Snapshot.
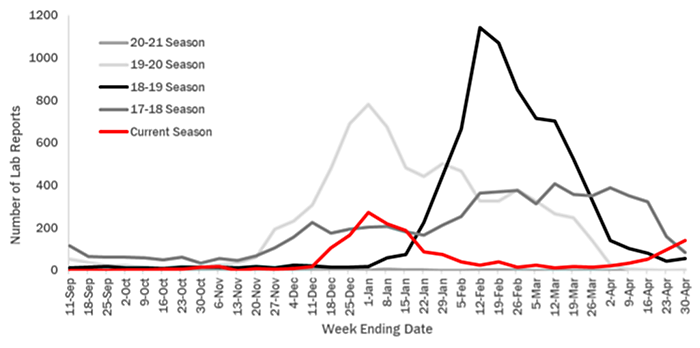
Positive influenza lab reports in Alaska by week of specimen collection for the 2017-2018 influenza season through present. The current season through April 30, 2022
Emergency Department Visits with COVID-like or Influenza-like Illness
- Syndromic surveillance consists of analyzing data on symptoms and diagnoses among patients visiting emergency departments in Alaska. The main goal is to identify trends. Unlike case-based surveillance, syndromic surveillance does not depend on laboratory testing.
- Influenza-like illness (ILI) is defined as having a fever and at least one other symptom, such as cough or sore throat. Patients with a diagnosis of influenza are also included, regardless of symptoms.
- COVID-like illness (CLI) encompasses a broader array of respiratory and other symptoms than influenza-like illness. This category also includes any patient with a diagnosis of COVID-19, regardless of symptoms.
- Patients with a diagnosis of COVID-19 are excluded from the ILI category and, likewise, patients with a diagnosis of influenza are excluded from the CLI category. But a patient without a diagnosis for either could be included in both the CLI and ILI categories. CLI and ILI may be caused by respiratory viruses other than SARS-CoV-2 and influenza virus.
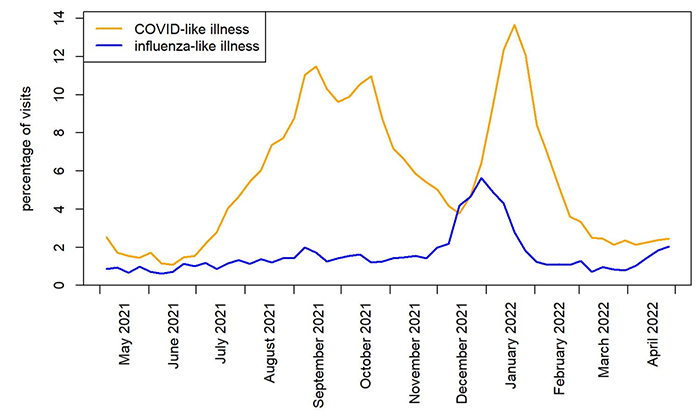
- As the Delta variant wave waned in Alaska in late October and November 2021, the percentage of emergency department patients with CLI declined. However, it increased in mid-December, reaching its peak in mid-January. Now, it is at a level lower than that observed in December before the Omicron wave. The percentage of emergency department patients with CLI the week of April 24–April 30 remained similar to the percentage recorded the prior week.
- ILI levels increased in December and peaked in late December 2021 and early January 2022. During April 2022, ILI levels increased again. The ILI level last week increased slightly from the percentage reported the previous week.
New updates to protect yourself and your family
-
The FDA limited the authorized use of the Johnson & Johnson vaccine. Individuals should only receive the Johnson & Johnson vaccine if they are aged 18+ and another authorized COVID-19 vaccine is not clinically appropriate or accessible given the rare (1 death pers 2 million doses give) but potentially fatal risk of thrombosis with thrombocytopenia or TTS. Learn more about who should receive a Johnson & Johnson vaccine here.
-
Treatments for COVID-19 are available and work best when given as soon as possible after symptoms start. If you test positive and you’re at increased risk for severe COVID-19, ask a health care provider about treatment options. If you have COVID-like symptoms but test negative on an at-home test, you could still have COVID-19. To be sure, either test again with an antigen test 2 days after your first test or consider getting a molecular test as soon as possible if you are at high-risk for complications. Learn more about COVID-19 treatments and where you can find COVID-19 treatments.
-
Vaccine boosters: Everyone 12 or older should get a COVID-19 vaccine booster if it's been five months since receiving the Pfizer or Moderna vaccines or two months since receiving the Johnson & Johnson vaccine. People over the age of 50 and some immunocompromised individuals may receive a second mRNA booster (Pfizer or Moderna) four months after their first booster dose. Additionally, people who have received the Johnson & Johnson vaccine for both their primary dose and booster dose may receive a second booster dose using an mRNA vaccine. Pfizer or Moderna vaccine boosters are preferred. Individuals aged 12-17 can receive a Pfizer booster only.
-
DHSS Community Case Rates: To complement the CDC’s Community Levels tool, DHSS introduced a new Community Case Rates tool. Both tools can help individuals, organizations, and communities make decisions about prevention measures. The Alert Levels on the dashboard has been retired and replaced by Community Case Rates.
-
Public transportation and masks: A federal court ruling has struck down the federal requirement to wear masks on public transit and at transportation hubs. Local authorities, airports, airlines, and other transportation companies may continue to enforce their own rules regarding masks. Check local or company rules before traveling. Alaskans are encouraged to consider current COVID-19 trends, personal risk factors, and other mitigation strategies in place when deciding where and when to wear a mask, and which kind to wear. Well-fitting, high-filtration masks such as N95 or KN95 masks offer the best protection.
Information and Resources
- The State of Alaska COVID-19 vaccines update page
- The State of Alaska COVID-19 information page provides more information about the virus and how individuals and businesses can protect themselves and others from transmission.
- The DHSS Business and Employer Toolkits page has communications resources for any organization that wants to keep workers, partners, clients, and customers informed about COVID-19.
- DHSS COVID-19 Communication Toolkit provides PSAs, flyers, and social media graphics.
- Learn more about the importance of physical activity, highlighted by our Play Every Day and our Healthy You 2022 campaigns: Play Every Day.
- Subscribe to the DHSS Insights blog for behind-the-scenes news about Alaska’s COVID-19 response and other efforts to protect the health and well-being of Alaskans.
- DHSS offers free presentations upon request to groups about COVID-19, the vaccines, COVID-19 prevention, or other health topics upon request. Learn more or request a presentation on our Speaker’s Bureau web page.
- For the most up-to-date case information, see the Alaska COVID-19 Information Hub dashboard: data.coronavirus.alaska.gov. All dashboard data are updated Wednesdays (except holidays).
ECHO sessions

Session information and recordings of previous ECHO sessions
subscribe to ECHO calendar updates | email: echo@alaskachd.org | website: akecho.org
ECHO sessions create virtual learning communities by connecting Alaska's health experts with specific audiences on specific topics. These sessions are produced and facilitated by UAA’s Center for Human Development Alaska ECHO project in partnership with the State of Alaska, Department of Health & Social Services.
Below is a selection of upcoming ECHO sessions. The full schedule of ECHO sessions and access to COVID-19 ECHO videos and slideshows are available for download anytime on the DHSS ECHO web page
School Health ECHO
Monday, 3-4 p.m., ending May 23rd (Register)
The School Health ECHO is a virtual learning network intended for professionals in the education setting (administrators, school-based nurses, etc.) to interface with a team of medical and education experts in Alaska.
Vaccine ECHO for Providers
Bi-weekly Tuesday, 2-3 p.m. (Register)
The Vaccine ECHO for providers provides planning and operation updates to vaccine providers across Alaska, while answering any questions you may have.
Public Science ECHO
Bi-weekly Wednesday, 12-12:45 p.m., ending May 25th (Register)
The Alaska Public Health Science ECHO is a virtual learning network intended for the general public to interface with our Public Health Leadership Team to explore the science of the COVID-19 virus, other public health topics, and current best practices. Or view via concurrent livestream to Facebook: https://www.facebook.com/akechoprograms
Healthcare Specific Situational Awareness ECHO
Bi-weekly Thursday, 1-2 p.m., ending May 26th (Register)
The Healthcare Specific Situational ECHO is a virtual learning network intended for healthcare professionals to interface with our Public Health Leadership Team to explore current best practices and the most recent information related to Public Health.
|
