COVID-19 Alaska Clinical Update – March 14
Monday, March 14
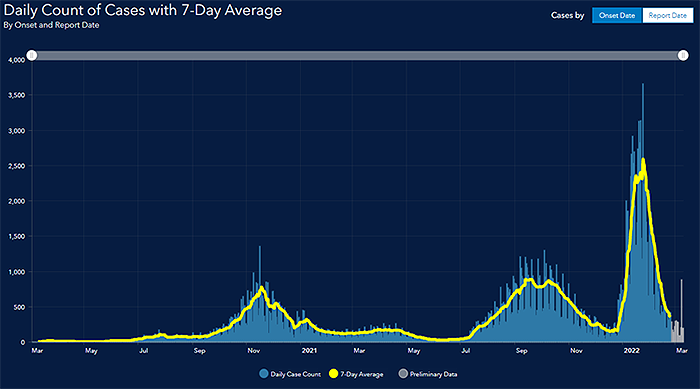
Graph taken from State of Alaska’s COVID-19 Cases Dashboard
Happy Pi day!
Updated mask guidance and COVID-19 Community Levels from the CDC
On February 25 the CDC released new mask guidance and links masking recommendations for the general public to the county’s COVID-19 community level. The COVID-19 community level metric considers 3 different calculations - new COVID-19 admissions per 100,000 population in the past 7 days, the percent of staffed inpatient beds occupied by COVID-19 patients, and total new COVID-19 cases per 100,000 population in the past 7 days. The CDC advises universal indoor masking, including in schools, only in counties with a “high” COVID-19 community level. In medium-risk communities, masking is recommended for those who are at an increased risk of severe disease. Others in medium- and low-risk communities may choose whether to wear a mask, regardless of vaccination status. These recommendations do not apply to healthcare settings. Because up to 15 boroughs and census areas may be contained in a single health service area in Alaska, DHSS is working to determine the strengths and limitations of the CDC Community Levels map for Alaska communities.
COVID-19 global death toll surpasses 6 million
According to the WHO’s global COVID-19 tracker on March 11, there have now been more than 6,025,000 deaths due to COVID-19 worldwide. In the United States there have been nearly 957,000 deaths. As of March 11, Alaska has officially reported 1,168 deaths attributed to COVID-19. However, the actual total of COVID-related deaths worldwide may be 2-4 times higher than the official number when global excess deaths are accounted for. According to CDC COVID-19 Seroprevelance Estimates, about 43% of the total US population have been infected with SARS-CoV-2 based on antibodies from natural infection, not vaccination.
Compounding these monumental losses, it is estimated that globally more than 5.2 million children lost a parent or caregiver during the first 19 months of the COVID-19 pandemic. Using data from more than 20 countries, researchers estimate the number of children experiencing COVID-19-associated orphanhood or caregiver death increased 90% from April 30 to October 31, 2021, from 2,737,300 to 5,200,300. Paternal orphans represented 76.5% of the orphaned children, compared to 23.5% who lost their mother. Beyond the tragic numbers, the study warns that children who lose a parent are at greater risk of poverty, sexual abuse, mental challenges, and severe stress.
In 2020, deaths during pregnancy or shortly after giving birth increased 14% from 2019
A new report from the US CDC National Center for Health Statistics shows that the number of women in the US who died during pregnancy or shortly after giving birth rose sharply during 2020, the first year of the pandemic. The data show that 861 women died of maternal causes in the US during 2020, an increase of 14% over the prior year. The maternal mortality rate increased to 23.8 deaths per 100,000 live births, up from 20.1 per 100,000 in 2019. Notably, the rate for non-Hispanic Black women was 2.9 times higher than the rate for non-Hispanic white women, a gap that increased between 2019 and 2020.
SARS-CoV-2 infection associated with lower survival rates for in-hospital cardiac arrest
Early on in the COVID-19 pandemic, investigators reported poor survival rates (<3%) after in-hospital cardiac arrest (IHCA) among patients with COVID-19 infection in the US and China, however these early studies were typically single-center studies with small sample sizes. This updated study used data from the American Heart Association Get With the Guidelines–Resuscitation (GWTG-R) registry, which contains detailed information on patients who experience cardiac arrest at participating hospitals in the United States. This study included 24,915 patients with IHCA from 286 hospitals who had a mean (SD) age of 64.7 (15.2) years. In terms of race and ethnicity, 6170 patients (24.8%) were Black, 15,223 (61.1%) were White, 949 (3.8%) were of other race or ethnicity (American Indian or Alaska Native, Asian or Pacific Islander, and other races and ethnicities), and 2573 (10.3%) were of unknown race or ethnicity. A suspected or confirmed COVID-19 infection was present in 5916 patients (23.7%). Patients with COVID-19 were younger, more frequently men and of Black race, and more likely to have an initial nonshockable rhythm, pneumonia, respiratory insufficiency, or sepsis and be receiving mechanical ventilation and vasopressors at the time of IHCA. Patients with COVID-19 and IHCA had lower rates of survival to discharge (11.9% vs 23.5%; adjusted RR, 0.65 [95% CI, 0.60-0.71]; P < .001) and ROSC (53.7% vs 63.6%; adjusted RR, 0.86 [95% CI, 0.83-0.90]; P < .001). They were also more likely to have received delayed defibrillation (27.7% vs 36.6%; RR, 1.30 [95% CI, 1.09-1.55]; P = .003) but not delayed epinephrine treatment. The association between COVID-19 infection and worse survival outcomes was consistent for patients with nonsurgical diagnoses, patients in the intensive care unit (ICU), and patients who had received timely defibrillation or epinephrine treatment. The absolute survival rate observed for US patients with IHCA and COVID-19 (11.9%) was higher than the survival rates reported initially (0-3.0%), which likely represented the isolated experience of health systems overwhelmed early during the pandemic. Although delays in resuscitation, especially defibrillation, may have contributed to lower survival, the negative association of COVID-19 with survival in this study was consistent across subgroups, including patients who received timely treatment with defibrillation and epinephrine.
More than 13% of people first tested positive for COVID 7 or more days after known exposure
In this retrospective cohort study that used data from 4 US universities between September 2020 to February 2021, 3641 university students and staff were identified as close contacts to individuals who tested positive for SARS-CoV-2 infection. Individuals were tested throughout the 10 to 14–day quarantine, and follow-up testing continued at least weekly throughout the 2020-2021 academic year. This study included 301 quarantined university students and staff who eventually tested SARS-CoV-2–positive (of 3641 quarantined total). These 301 individuals had a median (IQR) age of 22.0 (20.0-25.0) years; 131 (43.5%) identified as female; and 20 (6.6%) were staff. Of the 301 participants, 40 (13.3%; 95% CI, 9.9%-17.6%) had negative test results and were asymptomatic on day 7 compared with 15 (4.9%; 95% CI, 3.0%-8.1%) and 4 (1.4%; 95% CI, 0.4%-3.5%) on days 10 and 14, respectively. The 13.3% post–day 7 conversion rate implies that 13% of transmission may occur after release from 7-day quarantine. Quarantine length is a balance: a short quarantine brings increased risk of transmission from individuals who are infectious after release, while a long one may increase transmission risk by reducing compliance, stretching public health systems, and imposing additional economic and psychological hardship. To limit postquarantine transmission risk to 5% of total risk in a pre–Alpha variant university setting, the data from this study suggest that quarantine with RT-qPCR testing 1 day before intended release would need to extend to 10 days for nonstrict quarantine (possible interactions with household members) and 8 days for strict quarantine (dedicated housing, provided meals, provided linens/laundry, no personal interactions).
CDC updates list of high-risk medical conditions for severe COVID-19 outcomes
On February 24 the CDC updated the list of underlying medical conditions that are associated with a higher risk for severe COVID-19 outcomes. Additional disabilities included within this list are primary immunodeficiency and physical inactivity. The resources contain summarized data used to inform the findings, an explanation of the review process, and a list of actions that health professionals can take to care for their patients.
Alaska Influenza Snapshot – February 27 – March 5, 2022
The State of Alaska DHSS Section of Epidemiology publishes a weekly snapshot of influenza surveillance and activity during the flu season. The report from Week 9: February 27, 2022 – March 5, 2022 was recently published.
CPT1A Arctic Variant Refresher
The CPT1A Arctic Variant is a genetic mutation that is commonly in many Alaska Native people. Among the Yu’pik and Inupiaq Alaska Native people it is the most common form of CPT1A. During an illness where children have reduced fluid and caloric intake, children with CPT1A Arctic Variant are at increased risk of hypoglycemia, seizures, and death. ANTHC has published a brief video explaining this condition for physicians, other health care providers, and anyone else interested. In addition, Dr. Matthew Hirschfeld, Medical Director of Maternal Child Health Services at Alaska Native Medical Center, has published slides from a recent presentation he gave on CPT1A Arctic Variant and COVID-19 in Kids.
Caring for women Veterans in the community
Women Veterans are the fastest growing Veteran population in the VA healthcare system. They have unique health care needs that may require different assessments, care and resources compared to non-Veterans. For example, issues such as military sexual trauma, musculoskeletal pain, and post-deployment readjustment can impact women Veterans differently. To get the highest-quality care, women Veterans must have access to clinicians who are trained in women Veteran’s health. Community providers might not be aware of the special areas of concern that need to be addressed. To this end, the VA’s Office of Women’s Health has created a one-hour web-based training module “Caring for Women Veterans” which trains community care clinicians to provide Veteran and gender-specific care. Community Care Providers can take this training (CME available) and learn ways to talk about patients’ military history and address physical, mental, and reproductive health challenges unique to women Veterans.
MMWRs
COVID-19–associated hospitalization rates among children and adolescents aged 0–17 years increased rapidly in late December 2021, especially among children aged 0–4 years
This MMWR presents hospitalization data from the Coronavirus Disease 19–Associated Hospitalization Surveillance Network (COVID-NET) to describe COVID-19–associated hospitalizations among U.S. children (aged 0–11 years) and adolescents (aged 12–17 years) during periods of Delta (July 1–December 18, 2021) and Omicron (December 19, 2021–January 22, 2022) predominance. Complete clinical data were available for 1,834 and 266 hospitalized children and adolescents in the Delta-predominant and Omicron-predominant periods, respectively. During the Delta- and Omicron-predominant periods, pediatric weekly hospitalization rates peaked during the weeks ending September 11, 2021, and January 8, 2022, respectively; the Omicron variant peak (7.1 per 100,000 children and adolescents) was four times that of the Delta variant peak (1.8). Hospitalization rates among children aged 0–4 years were approximately five times as high during the peak week of the Omicron period (15.6) than during the Delta period (2.9) (RR [rate ratio] = 5.4; 95% CI = 4.0–7.2); RRs were also increased among children aged 5–11 years (Delta = 1.1; Omicron = 2.4; RR = 2.3; 95% CI = 1.5–3.6) and adolescents aged 12–17 years (Delta = 1.7; Omicron = 5.9; RR = 3.5; 95% CI = 2.5–5.0). Peak ICU admission rates for children and adolescents were 1.4 times higher during Omicron predominance (1.5) than during Delta predominance (1.1). During December 2021, when both variants were circulating, the rates of hospitalization were 23.5 and 3.8 per 100,000 among unvaccinated and fully vaccinated adolescents, respectively (RR = 6.3; 95% CI = 4.4–8.6)..The proportions of hospitalized children and adolescents requiring ICU admission (Delta = 27.8%; Omicron = 20.2%) or invasive mechanical ventilation (Delta = 6.3%; Omicron = 2.3%) were significantly lower during the Omicron period. A significantly higher proportion of unvaccinated adolescents were admitted to the ICU (30.3%) than were those who were vaccinated (15.5%).During July 1–December 31, 2021, 42.4% of hospitalized unvaccinated adolescents were non-Hispanic Black adolescents.
Between 5 and 9 days after symptom onset or after initial diagnosis with SARS-CoV-2 infection, 54% of persons had positive SARS-CoV-2 antigen test results. The proportion of positive results declined over time
Using data from the YKHC, this MMWR describes the prevalence of positive antigen tests 5-9 days after symptom onset or initial diagnosis of COVID infection in one Alaska region. On January 5, 2022, the Yukon-Kuskokwim Health Corporation (YKHC) recommended that persons with SARS-CoV-2 infection isolate for 10 days after symptom onset (or, for asymptomatic persons, 10 days after a positive nucleic acid amplification or antigen test result). However, isolation could end after 5–9 days if symptoms were resolving or absent, fever was absent for ≥24 hours without fever-reducing medications, and an Abbott BinaxNOW COVID-19 Ag (BinaxNOW) rapid antigen test result was negative. Antigen test results and associated individual characteristics were analyzed among 3,502 infections reported to YKHC during January 1–February 9, 2022. After 5–9 days, 396 of 729 persons evaluated (54.3%) had a positive antigen test result, with a declining percentage positive over time. In a multivariable model, a positive antigen test result was more likely after 5 days compared with 9 days (adjusted odds ratio [aOR] = 6.39) or after symptomatic infection (aOR = 9.63), and less likely after previous infection (aOR = 0.30), receipt of a primary COVID-19 vaccination series (aOR = 0.60), or after both previous infection and receipt of a primary COVID-19 vaccination series (aOR = 0.17). A positive antigen test was more likely after a symptomatic infection (361 of 564, 64.0%) than after an asymptomatic infection (35 of 165, 21.2%) (p<0.001). The proportion of positive antigen test results declined with the number of days since an initial positive test (p<0.001), and, among persons with symptomatic infections, since symptom onset (p<0.001). A positive test result was more likely if there was no history of previous infection (346 of 584, 59.2%) than if there was a documented previous infection (50 of 145, 34.5%) (p<0.001). Persons are estimated to be most infectious approximately 4 days after SARS-CoV-2 infection, and SARS-CoV-2 virus generally can be cultured up to 10 days after symptom onset. Rapid antigen test results have previously been shown to correlate with real-time reverse transcription–polymerase chain reaction cycle threshold values, and with detection of viable virus, for several days after infection.
COVID-19 vaccination coverage lower in rural than urban areas; gap widening since April 2021
To better understand COVID-19 vaccination disparities between urban and rural populations, CDC analyzed county-level vaccine administration data among persons aged ≥5 years who received their first dose of any of the 3 available COVID-19 vaccines during December 14, 2020–January 31, 2022, in 50 states and the District of Columbia (DC). COVID-19 vaccination coverage with ≥1 doses in rural areas (58.5%) was lower than that in urban counties (75.4%) overall, with similar patterns across age groups and sex. Coverage with ≥1 doses varied among states: 46 states had higher coverage in urban than in rural counties, one (Arizona) had higher coverage in rural than in urban counties. Three states and DC had no rural counties; thus, urban-rural differences could not be assessed. COVID-19 vaccine primary series completion was higher in urban than in rural counties. However, receipt of booster or additional doses among primary series recipients was similarly low between urban and rural counties. During December 14, 2020–April 10, 2021, urban-rural differences in first-dose COVID-19 vaccination coverage among adults aged ≥18 years were 6.8 percentage points; this gap has increased more than twofold to 16.9 percentage points in the current analysis among persons aged ≥5 years.
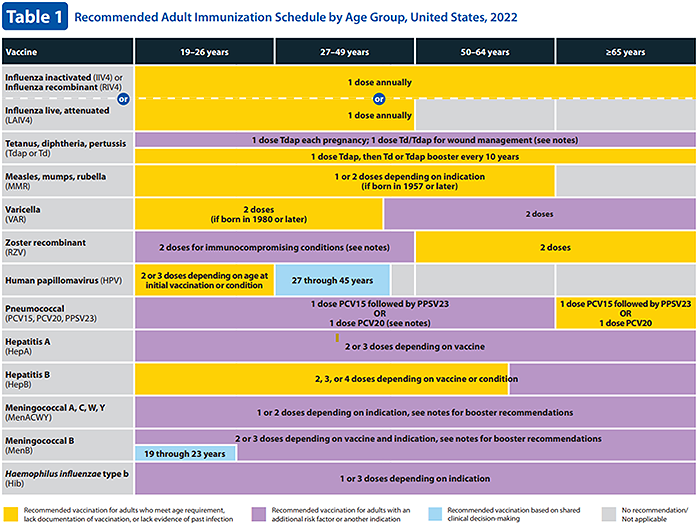
ACIP updates recommended immunization schedule for adults aged 19 years or older
At its November 2021 meeting, the Advisory Committee on Immunization Practices (ACIP) approved the Recommended Adult Immunization Schedule for Ages 19 Years or Older, United States, 2022. Vaccine-specific changes in the 2022 immunization schedule for adults aged ≥19 years include new or updated ACIP recommendations for hepatitis B vaccine (HepB), influenza vaccine, pneumococcal vaccines, recombinant zoster vaccine (RZV), and COVID-19 vaccine. Changes have also been made to the human papillomavirus (HPV); measles, mumps, and rubella (MMR); meningococcal; and varicella (VAR) vaccination sections to improve clarity in the language. In addition, an appendix listing the contraindications to and precautions for each vaccine has been added to the schedule this year.
RECURRENT TOPICS
Providing COVID-19 vaccinations
All Alaskans and people who work or live in Alaska who are aged 5 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Free self-paced online course available to promote COVID-19 vaccine confidence in Alaskan Communities
Two online course are available for free through the UAA Alaska Center for Rural Health & Health Workforce in partnership with the State of Alaska Department of Health and Social Services Division of Public Health. These courses are designed to provide participants the knowledge and skills to promote COVID-19 vaccine confidence among clients, family, friends, patients and/or community members in Alaskan communities. For those who complete the online course, there is an option to attend the live practical session to apply what they learned. These will occur monthly until the end of June and the live sessions are also free.
The Provider course is designed for licensed, or license eligible healthcare providers (1 contact hour, Interprofessional Continuing Education credit [ANMC]).
The Community course is aimed at entry level healthcare professionals and the interested public (approximately 3 hours)
Oral COVID-19 Antivirals
The FDA has authorized two novel oral antivirals – Paxlovid and Molnupiravir - for the treatment of mild-to-moderate COVID-19 in adults and children 12 years and older who are at high risk for progression to severe COVID-19.
The Alaska DHSS website on COVID-19 therapeutics has been updated for providers and has everything you need to evaluate which therapeutic is right for your patient and the tools to prescribe these medications.
Monoclonal Antibodies
Currently, only GlaxoSmithKline’s sotrovimab and Eli Lilly’s bebtelovimab monoclonal antibodies show high activity against the Omicron variant. Both are approved to treat mild-moderate COVID-19 in individuals who are at high risk for progression to severe COVID-19.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the NIH COVID-19 Treatment Guidelines
Pregnancy
The CDC strongly recommends COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology. In addition, JAMA has published a one-page patient information sheet on COVID-19 and pregnancy.
Post-acute Sequelae of COVID-19 (PASC)
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 in Alaska.
Aside from COVID-19
Opioids in Alaska
DHSS OSMAP Project HOPE are conducting public naloxone trainings as a community outreach and to increase awareness and access. Email projecthope@alaska.gov.
The Alaska Native Tribal Health Consortium (ANTHC) HIV/STD Prevention and Substance Misuse Prevention programs host free virtual gatherings to discuss harm reduction strategies and resources in Alaska. Guest speakers are Alaska-based experts in the field of harm reduction. Recordings of harm reduction trainings can be found here.
Several useful materials specific to Alaska opioid safety are at the following webpage. Check it out and print out information to hang up in your community.
Upcoming Events/Conferences/Presentations
Drug Addiction Treatment Act (DATA) Waivers ECHO
UAA Center for Human Development and the State of Alaska Division of Behavioral Health are pleased to offer a new Project ECHO for medical providers who are currently DATA waivered and/or medical providers who are interested in obtaining a DATA waiver.
April 13 at 12:00pm All things UDS/oral fluid tests for monitoring
May 11 at 12:00pm Behavioral Health - Psychosocial adjuncts to MAT
June 8 at 12:00pm Polysubstance use
July 13 at 12:00pm Tapering or stopping buprenorphine treatment
August 10 at 12:00pm Prenatal/OB MAT
Sept 14 at 12:00pm Understanding and reducing buprenorphine diversion
Registration link for DATA Waivers ECHO:
https://echo.zoom.us/meeting/register/tJYqce-gqDovGdDitNu5EPxMU1UOPrBth7Wv
Hosted and facilitated by UAA’S Center for Human Development Alaska ECHO Project in partnership with the State of Alaska Division of Behavioral Health. For questions, please contact echo@alaskachd.org
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule and the Zoom link.
March 18: Brian McMahon, MD. ANTHC Hepatology. NAFLD.
March 25: Ruby Fried, PhD. UAA Institute for Circumpolar Health Studies. COVID-19 Vaccine Acceptance and Hesitancy in Remote Alaska: A longitudinal perspective
April 1: Emily Urlacher. State of Alaska DHSS. Universal Developmental Screening Advisory Committee (UDSAC) Statewide Developmental Screening Environmental Scan.
April 8: Connie Jessen, MA. Alaska Indigenous Research Program Director. Alaska Stigma Index Project.
April 15: Eric Lim, MD. ANMC Orthopedics. Topic TBD
April 22: Leslie Kerzner, MD. Massachusetts General Hospital/Harvard Medical School. Neonatal Abstinence Syndrome for the Primary Care Provider.
April 29: Andrew Cornelius, MD. ANMC Orthopedics. Topic TBD.
May 6: Jessie Downes, MSN, DNP, RN. Alaska DHSS. Alaska Hypertension Program
Webinar Link: https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One-tap mobile: +16699006833,,98667611681#
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
The most up-to-date, evidence based COVID-19 treatment guidelines can be found at:
NIH COVID-19 Treatment Guidelines
IDSA Guidelines on the Treatment and Management of Patient with COVID-19
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
|
