COVID-19 Alaska Clinical Update
Tuesday, January 25, 2022
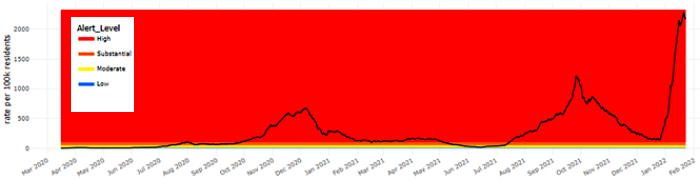
7-Day COVID-19 Case Rate – Statewide
Please help us improve this newsletter by answering a brief survey
Federal government expanding availability of at-home antigen tests and N95 masks
Every residential address in the US is now eligible to receive four free at-home rapid COVID antigen tests following the federal government’s recent purchase of one billion tests. Beginning on January 19, people may order tests online at COVIDTests.gov and the tests will typically ship within 7-12 days of ordering. In addition, the federal government will make 400 million nonsurgical N95 masks available for free at “thousands of locations,” namely pharmacies, supermarkets, and community health centers, across the country. The masks will come from the Strategic National Stockpile and White House officials hope to have the program fully operational by early February.
Remdesivir authorized for outpatient treatment of patients with mild to moderate COVID-19 at risk for progression to severe COVID-19
On January 21, the FDA expanded the approved indication and the EUA for remdesivir to be used for patients weighing at least 3.5kg (7.7lbs) with positive results of direct SARS-CoV-2 viral testing, and who are not hospitalized and have mild-to-moderate COVID-19, and are at high risk for progression to severe COVID-19, including hospitalization of death. This medication is administered as an IV infusion for three days and can be administered at an infusion center, skilled nursing facility, or home healthcare setting.
Early remdesivir resulted in 87% lower risk of hospitalization or death than placebo
From September 2020-Aril 2021, investigators ran a randomized, double-blind, placebo-controlled trial involving nonhospitalized patients with Covid-19 who had symptom onset within the previous 7 days and who had at least one risk factor for disease progression (age ≥60 years, obesity, or certain coexisting medical conditions) who were randomized to receive either 3 days of remdesivir infusions as an outpatient or placebo. A total of 562 patients who underwent randomization and received at least one dose of remdesivir or placebo were included in the analyses: 279 patients in the remdesivir group and 283 in the placebo group. The most common coexisting conditions were diabetes mellitus (61.6%), obesity (55.2%), and hypertension (47.7%). Covid-19–related hospitalization or death from any cause occurred in 2 patients (0.7%) in the remdesivir group and in 15 (5.3%) in the placebo group (hazard ratio, 0.13; 95% confidence interval [CI], 0.03 to 0.59; P=0.008). A total of 4 of 246 patients (1.6%) in the remdesivir group and 21 of 252 (8.3%) in the placebo group had a Covid-19–related medically attended visit by day 28 (hazard ratio, 0.19; 95% CI, 0.07 to 0.56). No patients had died by day 28. Adverse events occurred in 42.3% of the patients in the remdesivir group and in 46.3% of those in the placebo group. Among nonhospitalized patients who were at high risk for Covid-19 progression, a 3-day course of remdesivir had an acceptable safety profile and resulted in an 87% lower risk of hospitalization or death than placebo.
CDC strengthens recommendation for N95 and KN95 respirators
Last week the CDC updated its guidance on masks for the general public to say that people “may choose” to wear N95 and KN95 masks because these respirators “provide the highest level of protection from particles, including the virus that causes Covid-19.” For the first time, the CDC also said that “loosely woven cloth [masks] provide the least protection” against the SARS-CoV-2 virus.
FDA revokes EUA for bamlanivimab/etesevimab and REGEN-COV monoclonal antibody therapies since they are “unlikely to be active against the omicron variant”
On January 24 the FDA updated the EUA fact sheets for bamlanivimab/etesevimab and REGEN-COV to say that, “because data show these treatments are highly unlikely to be active against the omicron variant, which is circulating at a very high frequency throughout the United States, thesse treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time.” While this may change in the future depending on these treatments’ activity against novel variants, the federal Office of the Assistant Secretary for Preparedness and Response has halted allocations of these medications.
COVID-19 Therapeutics in Alaska
On January 7, DHSS sent a letter to the state’s healthcare providers and tribal health partners detailing the current availability and indicated use for monoclonal antibodies, novel oral antiviral medications, and remdesevir for the treatment of COVID-19. There is extremely limited supply, both nationally and in Alaska, of all current treatments and they are only indicated for those who are at risk for severe illness from COVID-19.
Updated Crisis Care Committee Recommendations for COVID-19 Therapeutics
The Alaska DHSS Crisis Care Committee has released updated therapeutics prioritization. This guidance is based on the NIH criteria but slightly modified for Alaska-specific considerations. The State is currently using tier 1a and 1b therapeutics.
FDA reiterates that antigen test swabs are for the nose only
After rumors circulated on social media earlier this month, the FDA announced that at-home rapid antigen test swabs should only be used “as directed” and the swabs in these kits are intended only to be used to collect samples from the nose and not from the back of the throat. The FDA says there is no “data yet suggesting throat swabs are an accurate or appropriate method for at-home tests.” These rumors began to appear after the FDA’s report in late December that preliminary studies evaluating the performance of some antigen tests using live virus samples from patients suggest that “antigen tests do detect the omicron variant but may have reduced sensitivity.”
UK reports decreased risk of hospitalization and vaccine efficacy rates for omicron variant
In a report from December 31, the UK’s Health Security Agency published data from two studies of the association between the omicron variant, vaccination status, and the risk of hospitalization. The studies found a lower overall risk of hospitalization with Omicron compared to Delta and a “substantial reduction in risk” of hospitalization for Omicron after 3 doses of vaccine compared to those who are unvaccinated. One study found that the risk of requiring emergency care or hospital admission with Omicron was approximately half of that for Delta and risk of hospital admission from emergency departments with Omicron was approximately one-third of the risk for Delta. This study also found an 65% and 81% reduction in the risk of hospitalization from Omicron after 2 and 3 doses of vaccine, respectively, compared to the unvaccinated. The second study reported a 68% reduction in the risk of hospitalization from Omicron after 3 doses of vaccine compared to the unvaccinated.
Omicron infections in California were associated with reduced risk of severe COVID-19 and short hospitalizations than Delta infections
In this large cohort study from the Kaiser Permanente Southern California healthcare system from November 30, 2021 to January 1, 2022, researchers compared disease severity and clinical outcomes for Omicron and Delta SARS-CoV-2 infections. This study included 52,297 cases of Omicron and 16,982 cases of Delta infections. Hospital admissions occurred among 235 (0.5%) and 222 (1.3%) of cases with Omicron and Delta variant infections, respectively. Among cases first tested in outpatient settings, the adjusted hazard ratios for any subsequent hospital admission and symptomatic hospital admission associated with Omicron variant infection were 0.48 (0.36-0.64) and 0.47 (0.35-0.62), respectively. Rates of ICU admission and mortality after an outpatient positive test were 0.26 (0.10-0.73) and 0.09 (0.01-0.75) fold as high among cases with Omicron variant infection as compared to cases with Delta variant infection. Zero cases with Omicron variant infection received mechanical ventilation, as compared to 11 cases with Delta variant infections throughout the period of follow-up. Median duration of hospital stay was 3.4 (2.8-4.1) days shorter for hospitalized cases with Omicron variant infections as compared to hospitalized patients with Delta variant infections, reflecting a 69.6% (64.0-74.5%) reduction in hospital length of stay.
No long-term effects on fertility from COVID-19 vaccination; possible short-term decline in male fertility associated with COVID-19 infection
In a prospective cohort study of 2,126 females in the US and Canada from December 2020-November 2021, researchers assessed the fertility of these females, their partners, and the potential impact of infections with SARS-CoV-2 or COVID-19 vaccination on fertility. COVID-19 vaccination was not appreciably associated with fertility in either partner (female fecundability ratio=1.08, 95% CI: 0.95, 1.23; male FR=0.95, 95% CI: 0.83, 1.10). Female SARS-CoV-2 infection was not strongly associated with fertility (FR=1.07, 95% CI: 0.87, 1.31). Male infection was associated with a transient reduction in fecundability (FR=0.82, 95% CI: 0.47, 1.45 for infection within 60 days; FR=1.16, 95% CI: 0.92, 1.47 for infection >60 days). These findings indicate that male SARS-CoV-2 infection may be associated with a short-term decline in fertility and that COVID-19 vaccination does not impair fertility in either partner.
Post-vaccine COVID antibodies persist in breast milk for up to 6 months
In this prospective longitudinal study of 30 pregnant or lactating women, SARS-CoV-2 antibody levels and neutralization capacity were analyzed at prevaccination, 1, 3, and 6 months post-vaccination. Human milk SARS-CoV-2-specific IgG levels peaked at 1 month postvaccination and persisted above prevaccination levels for at least 6 months. SARS-CoV-2-specific IgA was detected at 1 and 3 months (both P < .001) but waned by 6 months compared with baseline (P = .07). Milk SARS-CoV-2-specific IgG and IgA correlated with serum IgG at the same time point. Neutralization activity was seen in 83.3%, 70.4%, and 25.0% of milk samples at 1, 3, and 6 months postvaccination.
Omicron cases may be infectious for several days before being detectable by rapid antigen tests
Authors describe a high-risk occupational case cohort of 30 individuals with daily testing during an Omicron outbreak in December 2021 that had discordant SARS-CoV-2 test results from RT-qPCR and rapid antigen tests. Based on viral load and transmissions confirmed through epidemiological investigation, most Omicron cases were infectious for several days before being detectable by rapid antigen tests (Abbott BinaxNow and Quidel QuickVue tests). Cases were included if they were receiving daily testing at the time of diagnosis, had paired SARS-CoV-2 quantitative RT-qPCR test results and rapid antigen test results on Day 0 or 1 relative to first positive specimen collection date and were excluded if missing a recent negative test. The primary outcome of interest was discordance between saliva PCR and nasal rapid antigen test results during the early period with viral load levels corresponding to infectious risk of transmission. On Days 0 and 1, all rapid antigen tests produced false-negative results, despite 28 of 30 pairs having infectious viral load within the range of confirmed Omicron transmissions in the cohort. The median time from first positive PCR to first detectable antigen positive was 3 days. After infection was detected, a subgroup (n=5) who received daily saliva PCR, nasal swab PCR, and nasal swab rapid antigen testing showed viral load peaked in saliva 1-2 days before nasal tests. All individuals in the cohort developed symptoms within two days of the first PCR positive test.
Israel offering 4th doses of COVID vaccine
Beginning on January 3, Israel became the first country to offer a fourth COVID vaccine to people age 60 and older and medical workers who had received their last shot at least four months ago. This followed the health ministry’s approval of a fourth dose for people who are immunosuppressed, and for residents and staff of nursing homes. Early results have been mixed with one large observational study reportedly showing improved protection following a fourth dose, while a smaller study showed that a fourth dose increased antibody levels but was only partially effective at preventing infection with Omicron. Data have not yet been released for either of these studies and neither study has been published yet in a peer-reviewed medical journal.
Morbidity and Mortality Weekly Reports (MMWR)
Compared to White and non-Hispanic patients, there was lower use of outpatient monoclonal antibody treatment among Black, Asian, and Other race and Hispanic patients with COVID-19
The COVID-19 pandemic has magnified longstanding health care and social inequities, resulting in disproportionately high COVID-19–associated illness and death among members of racial and ethnic minority groups. Using health data from 41 U.S. health care systems that participated in the National Patient-Centered Clinical Research Network (PCORnet), this study assessed receipt of medications for COVID-19 treatment by race (White, Black, Asian, and Other races [including American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, and multiple or Other races]) and ethnicity (Hispanic or non-Hispanic) from March 2020 – August 2021. A total of 5,918,199 patients in PCORnet health care systems were tested for SARS-CoV-2, and 805,276 (13.6%) test results were positive. Critical care was required by 3.4% of all persons with positive test results compared with 1.8% of those treated with mAb. Patients who were Black, Asian, or Other race received mAb 22.4%, 48.3%, and 46.5%, respectively, less often than did White patients. SARS-CoV-2 positive patients of Hispanic ethnicity received mAb 57.7% less often (pt<0.001) than did non-Hispanic patients. Relative disparities in dexamethasone receipt by race were not statistically significant; however, small but systematic temporal differences in dexamethasone receipt were observed among White inpatients and Black, and Asian inpatients (both pw<0.05). Hispanic inpatients were treated with dexamethasone 6.2% less often than were non-Hispanic inpatients and systematic temporal treatment differences were also observed (pw = 0.005). Black inpatients received remdesivir 9.3% more often (pt = 0.03) than did White inpatients. Asian, Other race, and Hispanic inpatients did not experience significant relative disparities or systematic temporal differences in remdesivir treatment compared with White and non-Hispanic inpatients. Large relative differences were noted for mAb treatment, yet absolute differences were small. Relative differences in treatment with dexamethasone and remdesivir were less apparent in hospital settings, which might be attributed to ease of medication access. Equitable receipt of outpatient treatments, such as mAb and antiviral medications, and implementation of prevention practices are essential to reducing existing racial and ethnic inequities in severe COVID-19–associated illness and death.
Persons aged <18 years with COVID-19 were more likely to receive a new diabetes diagnosis >30 days after infection than were those without COVID-19
Increases in the number of type 1 diabetes diagnoses and increased frequency and severity of diabetic ketoacidosis at the time of diabetes diagnosis have been reported in European pediatric populations during the COVID-19 pandemic. To evaluate the risk for any new diabetes diagnosis (type 1, type 2, or other diabetes) >30 days after acute infection with SARS-CoV-2, CDC estimated diabetes incidence among patients aged <18years with diagnosed COVID-19 from retrospective cohorts constructed using IQVIA health care claims data from March 1, 2020, through February 26, 2021, and compared it with incidence among patients matched by age and sex who did not receive a COVID-19 diagnosis during the pandemic, or who received a prepandemic non–COVID-19 acute respiratory infection diagnosis. Analyses were replicated using a second data source (HealthVerity; March 1, 2020–June 28, 2021) that included patients who had any health care encounter possibly related to COVID-19. In the IQVIA database, Diabetes risk was 166% higher in the COVID-19 group than in the non-COVID-19 group (HR = 2.66, 95% CI = 1.98–3.56) and 116% higher than in the prepandemic ARI group (HR = 2.16, 95% CI = 1.64–2.86). In the HealthVerity database, diabetes incidence was 31% higher among patients aged <18 years with COVID-19 (399 per 100,000 person-years) than among those without COVID-19 (304 per 100,000 person-years; HR = 1.31, 95% CI = 1.20–1.44). The observed association between diabetes and COVID-19 might be attributed to the effects of SARS-CoV-2 infection on organ systems involved in diabetes risk. COVID-19 might lead to diabetes through direct attack of pancreatic cells expressing angiotensin converting enzyme 2 receptors, through stress hyperglycemia resulting from the cytokine storm and alterations in glucose metabolism caused by infection, or through precipitation of prediabetes to diabetes. A percentage of these new diabetes cases likely occurred in persons with prediabetes, which occurs in one in five adolescents in the United States. Steroid treatment during hospitalization might lead to transient hyperglycemia; however, only 1.5%–2.2% of diabetes codes were for drug- or chemical-induced diabetes, with the majority of codes being for type 1 or type 2 diabetes. Alternatively, COVID-19 might have indirectly increased diabetes risk through pandemic-associated increases in body mass index, a risk factor for both serious COVID-19 illness and diabetes.
Vaccination with Pfizer-BioNTech vaccine reduced likelihood of MIS-C in children age 12-18 years by 91%
The effectiveness of 2 doses of Pfizer-BioNTech vaccine received ≥28 days before hospital admission in preventing MIS-C was assessed using a test-negative case-control design among hospitalized patients aged 12–18 years at 24 pediatric hospitals in 20 states during July 1–December 9, 2021. Patients were hospitalized at 24 participating sites in the Overcoming COVID-19 Network, a collaboration between CDC and approximately 70 pediatric hospitals nationwide to assess COVID-19 complications in children and young adults. Case-patients met CDC criteria for MIS-C, which included a clinically severe illness requiring hospitalization, temperature ≥100.4°F (38°C) for ≥24 hours or subjective fever, evidence of inflammation (demonstrated by elevated levels of inflammatory markers), involvement of two or more organ systems, no alternative plausible diagnosis, and current or recent SARS-CoV-2 infection, indicated by a positive result from an RT-PCR test, serologic test, or antigen test. Two hospitalized control groups included 1) patients with one or more symptoms consistent with COVID-19, but with a negative result from a SARS-CoV-2 RT-PCR or antigen test and 2) patients without symptoms compatible with COVID-19 who might or might not have received SARS-CoV-2 testing. The 28-day window was selected because MIS-C generally occurs approximately 2–6 weeks after SARS-CoV-2 infection, with most cases occurring by the fourth week. The 283 patients in the primary analysis included 102 MIS-C case-patients and 181 controls. The median age among all case-patients and controls was 14.5 years, and 58% had at least one underlying condition including obesity. COVID-19 vaccination coverage was approximately 5% among case-patients and 36% among controls. Among 102 MIS-C case-patients, five (5%) were fully vaccinated ≥28 days before hospitalization, and 97 (95%) were unvaccinated. Overall, 91 (89%) patients had cardiovascular involvement, 84 (82%) had gastrointestinal involvement, and 68 (67%) had hematologic involvement. Sixty-two (61%) were admitted to an intensive care unit, and 38 (37%) received life support during hospitalization, including invasive mechanical ventilation, vasoactive infusions, or ECMO. All 38 MIS-C patients requiring life support were unvaccinated; among these, nine patients required invasive mechanical ventilation, 35 received vasoactive infusions and one required ECMO. No deaths among these patients were reported. Hospital length of stay was similar among vaccinated and unvaccinated MIS-C patients (median = 5 days). Vaccine efficacy against MIS-C was 91% (95% CI = 78%–97%). This analysis lends supportive evidence that vaccination of children and adolescents is highly protective against MIS-C and COVID-19 and underscores the importance of vaccination of all eligible children.
Among more than 1.2 million vaccinated persons, severe COVID-19-associated outcomes or death were rare; risk factors for severe outcomes included age ≥65 years, immunosuppressed, and six other underlying conditions
Using data from 465 facilities in a large U.S. health care database, this study assessed the frequency of and risk factors for developing a severe COVID-19 outcome after completing a primary COVID-19 vaccination series with any of the three authorized COVID-19 vaccines. Severe COVID-19 outcomes were defined as hospitalization with a diagnosis of acute respiratory failure, need for noninvasive ventilation (NIV), admission to an intensive care unit (ICU) including all persons requiring invasive mechanical ventilation, or death (including discharge to hospice). Among 1,228,664 persons who completed primary vaccination during December 2020–October 2021, a total of 2,246 (18.0 per 10,000 vaccinated persons) developed COVID-19 and 189 (1.5 per 10,000) had a severe outcome, including 36 who died (0.3 deaths per 10,000). In this study, age ≥65 years, immunosuppression, diabetes, and chronic kidney, cardiac, pulmonary, neurologic, and liver disease were associated with higher odds for severe COVID-19 outcomes; all persons with severe COVID-19 outcomes after primary vaccination had at least one of these risk factors and 77.8% of those who died had four or more risk factors. Previous COVID-19 illness was associated with reduced odds of severe outcomes (aOR = 0.27; 95% CI = 0.09–0.84).
COVID-19 vaccination during pregnancy was not associated with preterm birth or small-for-gestational-age at birth
This observational retrospective study evaluated the association of COVID-19 vaccination in pregnant women and the risk of preterm birth or small-for-gestational-age at birth at eight sites in California, Colorado, Minnesota, Oregon, Washington, and Wisconsin. Primary outcomes were preterm birth, defined as birth <37 weeks’ gestation, and SGA at birth, defined as birthweight <10th percentile for gestational age compared with a U.S. reference population. The study included 46,079 (82.8%) single-gestation pregnancies ending in live birth. Among these, 10,064 pregnant women (21.8%) received ≥1 COVID-19 vaccine doses during pregnancy. First (or only) vaccine doses were received in the first trimester by 172 (1.7%) women, in the second trimester by 3,668 (36.5%), and in the third trimester by 6,224 (61.8%). Most women received mRNA vaccines, including 5,478 (54.4%) who received Pfizer-BioNTech and 4,162 (41.4%) who received Moderna vaccines; 424 (4.2%) received Janssen (Johnson & Johnson) vaccine. Among 9,640 women who received mRNA vaccines during pregnancy, 1,759 (18.2%) received 1 dose, and 7,881 (81.8%) received 2 doses. The overall prevalence of preterm birth and SGA at birth were 6.6 and 8.2 per 100 live births, respectively. COVID-19 vaccination during pregnancy was not significantly associated with increased risk for preterm birth overall (adjusted Hazard Ratio = 0.91; 95% CI = 0.82–1.01; p = 0.06) or SGA at birth (aHR = 0.95; 95% CI = 0.87–1.03; p = 0.24), or when stratified by mRNA vaccine dose number during pregnancy, compared with the risk in unvaccinated pregnant women. There also was no association with increased risk for preterm or SGA at birth when evaluating vaccination by trimester for the first (or only) vaccine dose.
These data add to the evidence supporting the safety of COVID-19 vaccination during pregnancy. To reduce the risk for severe COVID-19–associated illness, CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant (including those who are lactating), who are trying to become pregnant now, or who might become pregnant in the future. The absolute risk for severe morbidity associated with COVID-19 in pregnancy is low; however, women with symptomatic COVID-19 during pregnancy have a more than twofold increased risk for intensive care unit admission, invasive ventilation, and extracorporeal membrane oxygenation, and a 70% increased risk for death, compared with nonpregnant women with symptomatic infections.
RECURRENT TOPICS
Providing COVID-19 vaccinations
All Alaskans and people who work or live in Alaska who are aged 5 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Oral COVID-19 Antivirals
The FDA has authorized two novel oral antivirals – Paxlovid and Molnupiravir - for the treatment of mild-to-moderate COVID-19 in adults and children 12 years and older who are at high risk for progression to severe COVID-19.
On January 12, there was a CDC COCA Call, “What Clinicians Need to Know About the New Oral Antiviral Medications for COVID-19.” The presentation describes the recent EUAs and NIH treatment guidelines, patient prioritization, and resources for healthcare providers. Experts reviewed when to prescribe antiviral medications including patient assessment, how to have a risk-benefit discussion to address patient questions or concerns, and how to prioritize patients if medications are in short supply.
Monoclonal Antibodies
FDA revokes authorization for bamlanivimab/etesevimab and REGEN-COV because of inactivity against Omicron – See above (link)
Currently, only GlaxoSmithKline’s sotrovimab monoclonal antibody treatment shows high activity against this variant. Sotrovimab has been approved to treat mild-moderate COVID-19 in individuals who are at high risk for progression to severe COVID-19.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the NIH COVID-19 Treatment Guidelines
Pregnancy
The CDC strongly recommends COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology. In addition, JAMA has published a one-page patient information sheet on COVID-19 and pregnancy.
Post-acute Sequelae of COVID-19 (PASC)
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
Myocarditis
For the latest recommendations, check out the CDC webpage on myocarditis and COVID-19 vaccines
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 vaccines available in Alaska.
Aside from COVID-19
Opioids in Alaska
DHSS OSMAP Project HOPE are conducting public naloxone trainings as a community outreach and to increase awareness and access. Email projecthope@alaska.gov.
The Alaska Native Tribal Health Consortium (ANTHC) HIV/STD Prevention and Substance Misuse Prevention programs host free virtual gatherings to discuss harm reduction strategies and resources in Alaska. Guest speakers are Alaska-based experts in the field of harm reduction. On December 1st, there will be a harm reduction training focused on polysubstance use. Other recordings of past harm reduction trainings can be found here.
Several useful materials specific to Alaska opioid safety are at the following webpage. Check it out and print out information to hang up in your community.
Upcoming Events/Conferences/Presentations
Drug Addiction Treatment Act (DATA) Waivers ECH
|
Date
|
Time
|
Session
|
| Feb 9 |
12:00 p.m. |
Successful strategies for buprenorphine home inductions |
| Feb 23 |
12:00 p.m. |
Using extended-release monthly buprenorphine |
| Mar 9 |
12:00 p.m. |
Microdosing/macrodosing buprenorphine |
| Apr 13 |
12:00 p.m. |
All things UDS/oral fluid tests for monitoring |
| May 11 |
12:00 p.m. |
Behavioral Health - Psychosocial adjuncts to MAT |
| Jun 8 |
12:00 p.m. |
Polysubstance use |
| Jul 13 |
12:00 p.m. |
Tapering or stopping buprenorphine treatment |
| Aug 10 |
12:00 p.m. |
Prenatal/OB MAT |
| Sep 14 |
12:00 p.m. |
Understanding and reducing buprenorphine diversion |
Registration link for DATA Waivers ECHO
Hosted and facilitated by UAA’S Center for Human Development Alaska ECHO Project in partnership with the State of Alaska Division of Behavioral Health. For questions, please contact echo@alaskachd.org
2022 Alaska Public Health Summit – January 18-20, 2022
Registration is now open for the 2022 Alaska Health Summit VIRTUAL conference taking place from Tuesday, January 18, 2022 to Thursday, January 20, 2022. The Summit theme will be The Intersection of Public Health and Public Safety, reflecting a wide range of issues and events facing us today. This is the first time ALPHA has created a Summit around a public safety theme that will feature keynote speakers and panels addressing policing across Alaska, corrections and reentry, drug overdose response, inequities in transportation, and other public safety issues, all from a public health perspective.
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule for the fall and the Zoom link.
|
Date
|
Session
|
| 01/28 |
Amber Frasure, MS: Trauma Informed Care Mini-Series. Part 2: A Deeper Dive into the Signs and Symptoms of Psychological Trauma and Specific Strategies to "Trauma Inform" your Medical Practice |
| 02/04 |
Amber Frassure, MS: Trauma Informed Care Mini-Series. Part 3: Effectively Communicating with Patients Using Motivational Interviewing |
| 02/11 |
Mary Schneider, BS, REHS: State of Alaska Lead Surveillance Program |
| 02/18 |
Vasisht Srinivasan, MD: Updates in Stroke Management |
Join Zoom Meeting
https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One tap mobile
+16699006833,,98667611681#
2022 Alaska Public Health Summit – January 18-20, 2022
Registration is now open for the 2022 Alaska Health Summit VIRTUAL conference taking place from Tuesday, January 18, 2022 to Thursday, January 20, 2022. The Summit theme will be The Intersection of Public Health and Public Safety, reflecting a wide range of issues and events facing us today. This is the first time ALPHA has created a Summit around a public safety theme that will feature keynote speakers and panels addressing policing across Alaska, corrections and reentry, drug overdose response, inequities in transportation, and other public safety issues, all from a public health perspective.
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
AK Clinical Reminders — UPDATED January 14, 2022

These ECHO sessions are produced and facilitated by
UAA’s Center for Human Development Alaska ECHO project
in partnership with the State of Alaska, Department of Health & Social Services
Session information and recordings of previous ECHO sessions
subscribe to ECHO calendar updates | email: echo@alaskachd.org | website: akecho.org
Upcoming Session Highlights:
Special Pop-Up Session: Alaska Medical Provider ECHO
Tuesday, January 18th from 7-8pm
Join us for this special pop-up session of the Alaska Medical Provider ECHO featuring updates on COVID-19, including the Omicron variant and new Federal guidelines.
Alaska Perinatal ECHO
Monthly on 3rd Thursday from 6-7 p.m. Register
Next Session: Thursday, January 20th
Please join us for the next Perinatal ECHO on Newborn Hearing Screening January 20th from 6:00-7:00pm! The featured didactic presentation will be on Alaska Newborn Hearing Screening Updates and Recent Issues: Changes in the Statewide System of Care, by Annette Callies, BSW. As always, we will have ample time for case study presentations, audience Q&A, and discussion with presenters and the hub team.
Regular Series
Alaska Medical Provider ECHO (formerly COVID-19 for AK Healthcare Providers)
Monthly on the 1st Tuesday of the month from 7-8 pm
This ECHO aims to increase knowledge and share best practices among medical providers across Alaska as well as to increase access to information for those living in rural areas of the state.
School Health ECHO
Every Monday from 3:00-4:00 p.m Register
The School Health ECHO is a virtual learning network intended for professionals in the education setting (administrators, school-based nurses, etc.) to interface with a team of medical and education experts in Alaska.
Vaccine ECHO for Providers
Weekly on Tuesday from 2-3 p.m. Register
The Vaccine ECHO for providers provides planning and operation updates to vaccine providers across Alaska, while answering any questions you may have.
Palliative Care ECHO
Monthly on the first Tuesday from 12-1 p.m.
This monthly ECHO is for all Alaskan healthcare disciplines supporting patients with serious illness, and aims to provide support and up-to-date information regarding Palliative Care during this period of COVID-19.
Public Science ECHO
Weekly on Wednesday from 12-1 p.m. register via Zoom
The Alaska Public Health Science ECHO is a virtual learning network intended for the general public to interface with our Public Health Leadership Team to explore the science of the COVID-19 virus, other public health topics, and current best practices. Or view via concurrent livestream to Facebook: https://www.facebook.com/akechoprograms
Local Government Public Health ECHO
Monthly on the third Wednesday from 3-4 p.m. Register
The Local Government Public Health Analysis ECHO is a virtual learning environment intended for local Alaska government leaders to interact with the State Public Health Leadership team and focuses on pandemic mitigation tools available, and how to use them.
Long Term Care Facilities ECHO
Second Wednesday of the month from 4-5 p.m. Register
Please join other staff and administrators of Alaska’s assisted living homes and residential care facilities to gather, learn, share, and grow. COVID has disrupted the fabric of our daily life and we can always learn from each other as we adjust to the new normal.
Healthcare Specific Situational Awareness ECHO
Weekly on Thursday from 12-1 p.m. Register
The Healthcare Specific Situational ECHO is a virtual learning network intended for healthcare professionals to interface with our Public Health Leadership Team to explore current best practices and the most recent information related to Public Health.
Perinatal ECHO
Monthly on 3rd Thursday from 6-7 p.m. Register
The Alaska Perinatal ECHO is a virtual learning network intended for medical providers caring for pregnant patients and their newborns.
EMS ECHO
Monthly on the 1st and 3rd Wednesday 1-2 p.m Register
The EMS ECHO is a virtual learning network intended for Emergency Medical Services and related personnel in Alaska to amplify best practices. Sessions are topic-driven and typically include a guest presenter or a brief lecture with an interactive case or process discussion.
Co-Occurring Behavioral Health, Opioid and Stimulant Use Disorders ECHO
1st & 3rd Wednesdays from 12:00pm-1:00pm, November 3, 2021 - April 20, 2022
The Co-Occurring Behavioral Health (COBH), Opioid and Stimulant Use Disorders ECHO facilitates a virtual network for behavioral health providers to learn best practice care through real-time access to experienced subject matter experts and their peers. Each session includes a brief lecture, de-identified case presentation for participants to receive feedback on complex cases, and open discussion facilitated by an interdisciplinary team.
Data Waivers ECHO New ECHO!
2nd Wednesdays from 12:00pm-1:00pm, November 10, 2021 - September 14, 2022
The Data Waivers ECHO facilitates a virtual network for clinical providers to learn and implement best practices for offering buprenorphine and other medically assisted treatment (MAT) services under a data waiver. Each session includes a brief lecture, de-identified case presentation for participants to receive feedback on complex cases, and open discussion facilitated by an interdisciplinary team.
|
COVID-19 testing guidelines and test site locator
AK COVID-19 clinical hotline for physicians: 833-751-4212. Staffed 24/7.
8PM-8AM is for urgent/emergent questions only.
AK Responders Relief Line: 24/7 behavioral health for everyone working in healthcare
during the COVID-19 pandemic: 1-844-985-8275
|
