COVID-19 Alaska Clinical Update
Thursday, December 23, 2021
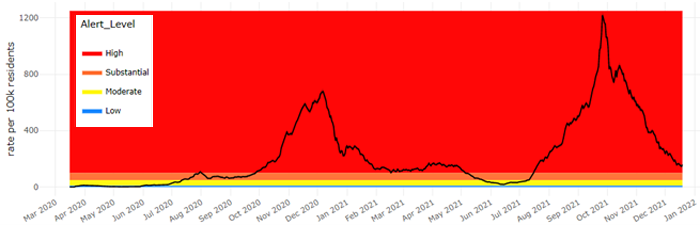
7-Day COVID-19 Case Rate – Statewide
Nationwide, Omicron accounts for more than 73% of total COVID infections
Based on the CDC’s published COVID variant reporting, as of December 18, the Omicron variant accounted for an estimated 73.2% of new SARS-CoV-2 infections reported from 12/11-12/18. The previous week it accounted for only 12.6% of all infections. As of publication, Alaska has still only identified one case of the Omicron variant in an Anchorage resident following international travel. However, genomic sequencing by the Alaska State Public Health Laboratory can take 2-3 weeks and additional cases may already be present though not yet detected.
The most recent Genomic Surveillance data can be found on the “COVID-19 Variants” tab of the Cases Dashboard.
Risk of reinfection with Omicron estimated to be 5.4x greater than risk of reinfection with Delta
A report from the Imperial College London COVID-19 response team estimates that the risk of reinfection with the Omicron variant is 5.4 times greater than that of the Delta variant. This implies that the protection against reinfection by Omicron afforded by past infection may be as low as 19%. Using data for all PCR-confirmed SARS-CoV-2 infections from November 29-December 11, authors estimate that the R0 for Omicron is “above 3” (R0 being the estimated number of people infected by each source patient). The study finds no evidence of Omicron having lower severity than Delta, judged by either the proportion of people testing positive who report symptoms, or by the proportion of cases seeking hospital care after infection. However, hospitalization data is very limited at this time. Controlling for vaccine status, age, sex, ethnicity, asymptomatic status, region and specimen date, Omicron was associated with a 5.40 (95% CI: 4.38-6.63) fold higher risk of reinfection compared with Delta. To put this into context, in the pre-Omicron era, the UK “SIREN” study of COVID infection in healthcare workers estimated that prior infection afforded 85% protection against a second COVID infection over 6 months. The reinfection risk estimated in the current study suggests this protection has fallen to 19% (95%CI: 0-27%) against an Omicron infection. Researchers found a significantly increased risk of developing a symptomatic Omicron case compared to Delta for those who were two or more weeks past their second vaccine dose, and two or more weeks past their booster dose (for AstraZeneca and Pfizer vaccines). The estimated vaccine efficacy against symptomatic Omicron infection is between 0% and 20% after two doses, and between 55% and 80% after a booster dose.
*This report has not gone through peer review and is not yet published in scientific journals. It may not be finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community. The paper is presented in the latest report from the WHO Collaborating Centre for Infectious Disease Modelling within the MRC Centre for Global Infectious Disease Analysis, Jameel Institute, Imperial College London.
Omicron case report raises concern for airborne transmission
An early release Research Letter from the CDC’s Emerging Infectious Diseases journal describes a case report of probable airborne transmission of an Omicron variant infection. This article summarizes the case of an Omicron variant infection in an asymptomatic, fully vaccinated traveler in a quarantine hotel in Hong Kong, China. The Omicron variant was also detected in a fully vaccinated traveler staying in a room across the corridor from the index patient, suggesting transmission despite strict quarantine precautions. Both patients had been fully vaccinated with the Pfizer-BioNTech vaccine, but neither had yet received boosters. Both case-patients tested negative by PCR within 72 hours before arrival. On arrival at the Hong Kong airport, both case-patients stayed in the same quarantine hotel and had rooms across the corridor from each other on the same floor. Case-patient A showed a positive COVID result without symptoms on November 13, 2021. He was hospitalized and isolated the next day. Case-patient B had mild symptoms develop on November 17, 2021. He showed a positive COVID result on November 18, 2021, and was hospitalized on the same day. Retrospective investigation, including closed-circuit television camera footage, confirmed that neither case-patient left their room during the quarantine period. No items were shared between rooms, and other persons did not enter either room. The only time the 2 quarantined persons opened their respective doors was to collect of food that was placed immediately outside each room door. The only other time they might have opened their doors would be for COVID tests, which were conducted in 3-day intervals, but since patients had arrived 1 day apart, it is unlikely that they would be tested on the same day. Airborne transmission across the corridor is the most probable mode of transmission.
Omicron variant outbreak in Norway restaurant gathering shows attack rate of 74%
In this case report, authors describe a cluster of Omicron variant cases associated with a company Christmas party held on November 26. Of the 110 attendees who were interviewed by investigators (117 total attendees at the party), 81 had positive PCR tests in the two weeks following the party. On November 26, the closed event was held in a separate room (ca 145 m2) in a restaurant in Oslo from 18:00 to 22:30, after which the venue was opened to the public from 22:30 to 03:00; attendees of the party mingled at the venue before and after dinner, following which the bar and dance area was opened to the public. All attendees of the party were reported to be fully vaccinated and had been asked by the organizer to perform a rapid antigen self-test. The total attack rate for the Omicron variant was 74% (81/110). Assuming exposure occurred at the party, the incubation period for symptomatic cases ranged from 0 to 8 days with a median of 3 days. One case was asymptomatic and 74 (91%) reported at least three symptoms. None of the cases required hospitalization by December 13, 2021. Most of the cases (n = 79; 98%) and non-cases (n = 27; 93%) were fully vaccinated with a median time since receiving the last vaccine dose of 79 days for cases and 87 days for non-cases. In addition, during the investigation and as at 13 December, authors detected nearly 70 other guests that were likely infected at the venue, and the Omicron variant was detected in 53 of these through PCR variant screening or sequencing.
Most currently available monoclonal antibodies expected to be ineffective against the Omicron variant; Sotrovimab appears to retain its efficacy
In a pre-print study that has not yet been peer reviewed, researchers tested currently available monoclonal antibody therapies (mAbs), plasma from vaccinated individuals, and convalescent plasma from individuals previously infected with COVID-19 against the Omicron variant in vitro. Omicron was totally or partially resistant to neutralization by all mAbs tested. Bamlanivimab+Etesevimab and REGEN-COV, two of the mAbs authorized in the US, were inactive against Omicron. Sotrovimab was the only antibody currently authorized in the US that displayed similar activity against both Delta and Omicron variants. Sera from Pfizer or AstraZeneca vaccine recipients sampled 5 months after complete vaccination barely inhibited Omicron. Sera from COVID-19 convalescent patients collected 6 or 12-months post symptoms displayed low or no neutralizing activity against Omicron. Administration of a booster Pfizer dose as well as vaccination of previously infected individuals generated an anti-Omicron neutralizing response, with titers 5-to-31-fold lower against Omicron than against Delta. The authors conclude that Omicron escapes most therapeutic monoclonal antibodies and to a large extent vaccine-elicited antibodies.
*This article has not gone through peer review and is in pre-print status. It may have not been finalized by authors, might contain errors, and report information has not yet been accepted or endorsed in any way by the scientific or medical community.
CDC/IDSA COVID-19 Clinician Call – Omicron overview and monoclonal antibody therapy update
On December 18, the CDC and Infectious Diseases Society of America hosted an expert panel discussion on the Omicron variant and updates on monoclonal antibody therapies. A recording of this presentation can be found at the following link.
US Assistant Secretary for Preparedness and Response pausing allocations of bamlanivimab+etesevimab and REGEN-COV because of decreased protection against Omicron variant
On December 22, the FDA updated the Health Care Provider Fact Sheets for bamlanivimab and etesevimab administered together, REGEN-COV, and sotrovimab with specific information regarding expected activity against the Omicron variant (B.1.1.529/BA.1). These data show that it is unlikely that bamlanivimab and etesevimab administered together or REGEN-COV will retain activity against this variant. Based on similar cell culture data currently available, sotrovimab appears to retain activity against the Omicron variant. Based on this information, The Assistant Secretary for Preparedness and Response will pause any further allocations of bamlanivimab and etesevimab together, etesevimab alone, and REGEN-COV pending updated data from the CDC.
FDA authorizes Pfizer’s Paxlovid, the first oral antiviral for treatment of COVID-19
On December 22, the FDA issued emergency use authorization for Pfizer’s Paxlovid (nirmatrelvir tablets and ritonavir tablets, co-packaged for oral use) for the treatment of mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kilograms or about 88 pounds) with positive results of direct SARS-CoV-2 testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death. Paxlovid is available by prescription only and should be initiated as soon as possible after diagnosis of COVID-19 and within five days of symptom onset. Paxlovid is not authorized for the pre-exposure or post-exposure prevention of COVID-19 or for initiation of treatment in those requiring hospitalization due to severe or critical COVID-19. The medication is administered as three tablets (two tablets of nirmatrelvir and one tablet of ritonavir) taken together orally twice daily for five days, for a total of 30 tablets. The primary data supporting Paxlovid comes from the EPIC-HR, a randomized, double-blind, placebo-controlled clinical trial studying Paxlovid for the treatment of non-hospitalized symptomatic adults with a laboratory confirmed diagnosis of SARS-CoV-2 infection. Patients were adults 60 years or older regardless of risk factors or 18 years of age and older with a prespecified risk factor for progression to severe disease. All patients had not received a COVID-19 vaccine and had not been previously infected with COVID-19. The main outcome measured in the trial was the proportion of people who were hospitalized due to COVID-19 or died due to any cause during 28 days of follow-up. Paxlovid significantly reduced the proportion of people with COVID-19 related hospitalization or death from any cause by 88% compared to placebo among patients treated within five days of symptom onset and who did not receive COVID-19 therapeutic monoclonal antibody treatment. In this analysis, 1,039 patients had received Paxlovid, and 1,046 patients had received placebo and among these patients, 0.8% who received Paxlovid were hospitalized or died during 28 days of follow-up compared to 6% of the patients who received placebo.
The State of Alaska will receive an extremely limited supply of this medication in the next few weeks and only a select few pharmacies will have the drug available initially. However, availability will expand to other sites when the State’s allocation increases.
FDA authorizes Merck’s Molnupiravir, another oral antiviral for treatment of COVID-19
On December 23, the FDA issued emergency use authorization for Pfizer’s Molnupiravir for the treatment of mild-to-moderate COVID-19 in adults with positive results SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death, and for whom alternative COVID-19 treatment options authorized by the FDA are not accessible or clinically appropriate. Molnupiravir is available by prescription only and should be initiated as soon as possible after diagnosis of COVID-19 and within five days of symptom onset. Molnupiravir is not authorized for use in patients younger than 18 years of age because the medication may affect bone and cartilage growth. It is not authorized for the pre-exposure or post-exposure prevention of COVID-19 or for initiation of treatment in patients hospitalized due to COVID-19 because benefit of treatment has not been observed in people when treatment started after hospitalization due to COVID-19. Molnupiravir is administered as four 200 milligram capsules taken orally every 12 hours for five days, for a total of 40 capsules. Molnupiravir is not authorized for use for longer than five consecutive days.
The State of Alaska will receive an extremely limited supply of this medication in the next few weeks and only a select few pharmacies will have the drug available initially. However, availability will expand to other sites when the State’s allocation increases.
Pfizer-BioNTech vaccine didn’t generate adequate immune response in children 2 to 5 years-old
On December 15, Pfizer-BioNTech announced that for its Phase 1/2/3 trial for children age 6 months to 5 years, it will be adding a third dose of 3 µg at least two months after the second dose of the two-dose series to provide high levels of protection in this young age group. In a pre-specified immunogenicity analysis one month following the second dose, immune responses in the 2 to 5 year-old were inferior to the immune responses seen in older children age 16-25. Non-inferiority was met for the 6- to 24-month-old population but not for the 2- to under 5-year-old population in this analysis. No safety concerns were identified and the 3 µg dose demonstrated a favorable safety profile in children 6 months to under 5 years of age. If the three-dose study is successful, Pfizer and BioNTech expect to submit data to regulators to support an Emergency Use Authorization (EUA) for children 6 months to under 5 years of age in the first half of 2022.
*These results have not gone through peer review and were announced in a press release by the sponsoring health insurance company. The results might contain errors and report information that has not yet been accepted or endorsed in any way by the scientific or medical community.
Percentage of adolescents reporting drug use decreased significantly in 2021
The percentage of adolescents reporting substance use decreased significantly in 2021, according to the latest results from the National Institute on Drug Abuse’s Monitoring the Future survey of substance use behaviors and related attitudes among 8th, 10th, and 12th graders in the United States. In line with continued long-term declines in the use of many illicit substances among adolescents previously reported by the Monitoring the Future survey, these findings represent the largest one-year decrease in overall illicit drug use reported since the survey began in 1975. This year, the study surveyed students on their mental health during the COVID-19 pandemic. The study found that students across all age-groups reported moderate increases in feelings of boredom, anxiety, depression, loneliness, worry, difficulty sleeping, and other negative mental health indicators since the beginning of the pandemic. This year, 11.3% of the students who took the survey identified as African American, 16.7% as Hispanic, 5.0% as Asian, 0.9% as American Indian or Alaska Native, 13.8% as multiple, and 51.2% as white. The percentage of students who reported using alcohol within the past year decreased significantly for 10th and 12th grade students (28.5% down from 40.7%, and 46.5% down from 55.5%, respectively) and remained stable for 8th graders (17.2%). The percentage of students who reported using marijuana (in all forms, including smoking and vaping) within the past year decreased significantly for 8th, 10th, and 12th grade students (7.1%, 17.3%, and 30.5%, respectively). Vaping continues to be the predominant method of nicotine consumption among young people, though the percentage of students who reported vaping nicotine within the past year decreased significantly for 8th, 10th, and 12th grade students (12.1%, 19.5%, and 26.6%, respectively). The percentage of students who reported using any illicit drug (other than marijuana) within the past year decreased significantly for 8th, 10th, and 12th grade students (4.6%, 5.1%, and 7.2%, respectively). Researchers detected shifts in the drugs used, with alcohol use declining and use of nicotine products and misuse of prescription medications increasing. Adolescents who experienced pandemic-related severe stress, depression, or anxiety, or whose families experienced material hardship during the pandemic, or whose parents used substances themselves were most likely to use them too.
CDC updates guidance for K-12 schools to allow for “test to stay” strategy following COVID exposure
On December 17, the CDC said unvaccinated students exposed to a person with COVID-19 can remain in school if they are tested twice in the week following exposure and both tests are negative – “Test to Stay”. The new guidance is an effort to keep children in school instead of having to quarantine at home and miss class, while also alleviating the burden on parents to arrange child care. The new protocol, which should be used as one method in a layered prevention approach, is based on two MMWR studies explained below.
Alaska Section of Epidemiology releases updated At-Home COVID-19 testing guidance
The Alaska Section of Epidemiology released its updated “Guidance for Coronavirus Disease 2019 (COVID-19) Testing in Alaska”, “Reporting COVID testing”, and new guidance for at-home COVID-19 tests. As of January 10, 2022, sites with a CLIA-waived status will be required to report positive results only.
Morbidity and Mortality Weekly Reports (MMWR)
“Test to stay” strategy in Illinois allowed masked students and staff with a COVID exposure to remain in school and preserved nearly 8,200 in-person learning days
In this MMWR, authors present evidence from the the Lake County Health Department (LCHD) in Illinois, which introduced a Test to Stay (TTS) strategy in August 2021, whereby unvaccinated students, teachers, and staff members with certain school-related COVID-19 exposures could remain in school and extracurricular activities if they wore masks, remained asymptomatic, and underwent COVID testing on days 1, 3, 5, and 7 after exposure. TTS participants were required to quarantine at home for 14 days while not attending school or participating in school-based activities. During August 9–October 29, 2021, 90 Lake County schools implemented TTS, representing 53.7% (6,267) of staff members and 53.4% (65,384) of public school students. During this period, 258 index COVID-19 patients and 1,664 close contacts were reported. Among TTS participants, 16 secondary cases were identified, all of whom were in students; no secondary cases were identified among staff members. Nearly all cases were in non-Hispanic White male students. The secondary attack risk (number of close contacts who received a positive SARS-CoV-2 test result within 14 days after exposure to an index patient, divided by total number of close contacts) was 1.5% (16 of 1,035). However, nine tertiary cases were identified among household contacts of the 16 secondary cases, and four of the nine were fully vaccinated. Assuming a maximum of 8 missed school days for every 10-day quarantine period, up to 8,152 in-person learning days were saved among TTS participants. Based on investigation interviews, the most common likely locations of COVID-19 exposure among TTS participants were school buses (56.3%), classrooms (32.4%), and school-sanctioned sports (7.4%). Secondary transmission was lowest in elementary schools (1.1%), followed by middle schools (1.3%) and high schools (4.9%). The findings in this report are subject to multiple limitations. First, inequity in school districts’ staffing and testing resources might have introduced selection bias because only schools with sufficient resources offered TTS. High-resource schools might have more staffing capacity and physical spacing to apply prevention strategies (e.g., distancing students), which might have resulted in low transmission levels that are not generalizable to low-resource schools. Second, data might not be generalizable to areas with higher COVID-19 incidences and lower vaccination rates. Third, 33% of parents did not respond to LCHD calls or might have chosen not to disclose exposures occurring outside school, resulting in students at high risk being incorrectly enrolled in TTS. This would likely have resulted in an overestimation of secondary transmission among TTS participants. Teachers and staff members had much lower participation rates than did students in this evaluation because of high vaccination rates, low number of exposures meeting close contact definition, and lack of awareness in some schools that adults could participate in TTS. Implementation of TTS with other concurrent prevention strategies, including masking and physical distancing, limited further spread of SARS-CoV-2 within K–12 schools and allowed students to safely sustain in-person learning.
“Test to stay” strategy in LA County did not lead to increase in COVID-19 transmission risk and reduced number of in-person school days lost
Similar to the MMWR above, in July 2021, 50 school districts in LA County adopted a Test-To-Stay (TTS) strategy which enabled unvaccinated students exposed in school to a person infected with SARS-CoV-2, to remain in school while under quarantine, if both the infected person and the exposed person wore masks correctly and consistently throughout the exposure. To stay in school during the quarantine period, the exposed student must remain asymptomatic, wear a mask at school, and undergo twice weekly testing for SARS-CoV-2. During September 20–October 31, among 78 school districts, 39 (50%) permitted TTS. These TTS schools constitute 21% of LAC public schools. Overall, within the 1,635 non-TTS schools, 4,322 COVID-19 cases occurred among 967,188 enrolled students (4.7 cases per 1,000 students); among 18,729 student close contacts, the secondary infection risk was 1.3%. Non-TTS districts lost an estimated 92,455 in-person school days during September 20–October 31 while students were in quarantine. Within the 432 TTS schools, among 324,879 enrolled students, 812 COVID-19 cases occurred (2.5 cases per 1,000 students); among 7,511 student close contacts, the secondary infection risk was 0.7%. As a result of the TTS protocol, no in-person school days were lost among quarantined students participating in TTS. TTS schools did not experience increases in COVID-19 incidence among students after TTS implementation, and in 20 identified outbreaks in TTS schools, no tertiary transmission was identified. Among the schools that implemented TTS, 107 of 410 (26%) were categorized as most disadvantaged compared with 1,192 of 1,619 (74%) non-TTS schools. Challenges cited to TTS implementation were limited staffing and systems to monitor mask use, testing, and lack of family support. Moreover, because TTS is currently permitted for quarantined students only during regular school hours, families who rely on before- and after-school programs might opt for home quarantine. Preliminary data from LAC suggest that a school-based TTS strategy in a large and diverse county did not increase school transmission risk and might greatly reduce loss of in-person school days.
Adults who had a healthcare provider recommend a COVID-19 vaccine were more likely to have received ≥1 dose of a COVID-19 vaccine than were those who did not receive a recommendation
Using data from the National Immunization Survey-Adult COVID Module (NIS-ACM), a nationally representative cell phone survey, authors report on the impact of a healthcare provider recommending COVID-19 vaccination. There was an overall sample size of 340,543 participants and the survey assessed report of health care provider recommendation for COVID-19 vaccination, COVID-19 vaccination status, and attitudes toward vaccination. The reported prevalence of a provider recommending COVID-19 vaccination increased from 34.6% (April 22–May 29), to 40.5% (August 29–September 25, 2021). Adults who reported a provider recommendation for COVID-19 vaccination were more likely to have received ≥1 dose of a COVID-19 vaccine (77.6%) than were those who did not receive a recommendation (61.9%). Provider recommendation was also associated with higher likelihood of receipt of ≥1 COVID-19 vaccine dose among most subgroups, with highest adjusted prevalence ratio (aPR) for younger adults aged 18-39 years (aPR = 1.22), non-Hispanic American Indian or Alaska Native adults (aPR = 1.19), adults living in rural areas (aPR = 1.18), adults living in the West or Midwest, and adults who did not have a school or work COVID-19 vaccination requirement (aPR = 1.15). In the jurisdiction-level correlation analysis, COVID-19 vaccination coverage was higher among persons living in jurisdictions with higher prevalence of provider recommendation. For example, in Wyoming, prevalence of report of a provider recommendation was 30.1%, and COVID-19 vaccination coverage was 51.2%, whereas in Puerto Rico, prevalence of provider recommendation was 50.5%, and COVID-19 vaccination coverage was 77.5%. Empowering health care providers to recommend vaccination to their patients could help reinforce confidence in, and increase coverage with, COVID-19 vaccines, particularly among groups known to have lower COVID-19 vaccination coverage, including younger adults, racial/ethnic minorities, and rural residents.
RECURRENT TOPICS
Providing COVID-19 vaccinations
All Alaskans and people who work or live in Alaska who are aged 5 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Pregnancy
The CDC strongly recommends COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology. In addition, JAMA has published a one-page patient information sheet on COVID-19 and pregnancy.
Monoclonal Antibodies
Three different monoclonal antibody treatments for COVID-19, have been authorized, however, due to concern about decreased efficacy against the Omicron variant, only sotrovimab is recommended at this time. For additional information, see above. GlaxoSmithKline’s sotrovimab has been approved to treat mild-moderate COVID-19 in individuals who are at high risk for progression to severe COVID-19.
Side-by-side overview of outpatient MAB therapies
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the CDC webpage on Monoclonal Antibodies for High-Risk COVID-19 patients and COVID-19 Monoclonal Antibody Resources for Healthcare Providers.
Ivermectin
Current evidence does not support the use of ivermectin for the treatment or prevention of COVID-19.
CDC - Health advisory about ivermectin
Cochrane Review - COVID-19 and ivermectin
FDA - Why you should not use ivermectin to treat or prevent COVID-19
Infectious Disease Society of America (IDSA) guidelines do not recommend ivermectin
Post-acute Sequelae of COVID-19 (PASC)
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
Myocarditis
For the latest recommendations, check out the CDC webpage on myocarditis and COVID-19 vaccines
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 vaccines available in Alaska.
Aside from COVID-19
Opioids in Alaska
DHSS OSMAP Project HOPE are conducting public naloxone trainings as a community outreach and to increase awareness and access. Email projecthope@alaska.gov.
The Alaska Native Tribal Health Consortium (ANTHC) HIV/STD Prevention and Substance Misuse Prevention programs host free virtual gatherings to discuss harm reduction strategies and resources in Alaska. Guest speakers are Alaska-based experts in the field of harm reduction. On December 1st, there will be a harm reduction training focused on polysubstance use. Other recordings of past harm reduction trainings can be found here.
Several useful materials specific to Alaska opioid safety are at the following webpage. Check it out and print out information to hang up in your community.
Upcoming Events/Conferences/Presentations
Drug Addiction Treatment Act (DATA) Waivers ECHO
UAA Center for Human Development and the State of Alaska Division of Behavioral Health are pleased to offer a new Project ECHO for medical providers who are currently DATA waivered and/or medical providers who are interested in obtaining a DATA waiver.
|
Date
|
Time
|
Session
|
| Jan 12 |
12:00 p.m. |
Preparing for your first OUD MAT visit |
| Feb 9 |
12:00 p.m. |
Successful strategies for buprenorphine home inductions |
| Feb 23 |
12:00 p.m. |
Using extended-release monthly buprenorphine |
| Mar 9 |
12:00 p.m. |
Microdosing/macrodosing buprenorphine |
| Apr 13 |
12:00 p.m. |
All things UDS/oral fluid tests for monitoring |
| May 11 |
12:00 p.m. |
Behavioral Health - Psychosocial adjuncts to MAT |
| Jun 8 |
12:00 p.m. |
Polysubstance use |
| Jul 13 |
12:00 p.m. |
Tapering or stopping buprenorphine treatment |
| Aug 10 |
12:00 p.m. |
Prenatal/OB MAT |
| Sep 14 |
12:00 p.m. |
Understanding and reducing buprenorphine diversion |
Registration link for DATA Waivers ECHO
Hosted and facilitated by UAA’S Center for Human Development Alaska ECHO Project in partnership with the State of Alaska Division of Behavioral Health. For questions, please contact echo@alaskachd.org
2022 Alaska Public Health Summit – January 18-20, 2022
Registration is now open for the 2022 Alaska Health Summit VIRTUAL conference taking place from Tuesday, January 18, 2022 to Thursday, January 20, 2022. The Summit theme will be The Intersection of Public Health and Public Safety, reflecting a wide range of issues and events facing us today. This is the first time ALPHA has created a Summit around a public safety theme that will feature keynote speakers and panels addressing policing across Alaska, corrections and reentry, drug overdose response, inequities in transportation, and other public safety issues, all from a public health perspective.
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule for the fall and the Zoom link.
|
Date
|
Session
|
| 01/14 |
Hope Finkelstein, Alaska FASD Program Manager: DHSS FASD Program |
| 01/21 |
Victoria Miller, MFA, LPC: Trauma Informed Care Mini-Series. Part 1: Early Life Adversity, Later Life Disease & Implications for Health Care |
| 01/28 |
Amber Frasure, MS: Trauma Informed Care Mini-Series. Part 2: A Deeper Dive into the Signs and Symptoms of Psychological Trauma and Specific Strategies to "Trauma Inform" your Medical Practice |
| 02/04 |
Amber Frassure, MS: Trauma Informed Care Mini-Series. Part 3: Effectively Communicating with Patients Using Motivational Interviewing |
| 02/11 |
Mary Schneider, BS, REHS: State of Alaska Lead Surveillance Program |
| 02/18 |
Vasisht Srinivasan, MD: Updates in Stroke Management |
Join Zoom Meeting
https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One tap mobile
+16699006833,,98667611681#
2022 Alaska Public Health Summit – January 18-20, 2022
Registration is now open for the 2022 Alaska Health Summit VIRTUAL conference taking place from Tuesday, January 18, 2022 to Thursday, January 20, 2022. The Summit theme will be The Intersection of Public Health and Public Safety, reflecting a wide range of issues and events facing us today. This is the first time ALPHA has created a Summit around a public safety theme that will feature keynote speakers and panels addressing policing across Alaska, corrections and reentry, drug overdose response, inequities in transportation, and other public safety issues, all from a public health perspective.
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
COVID-19 testing guidelines and test site locator
AK COVID-19 clinical hotline for physicians: 833-751-4212. Staffed 24/7.
8PM-8AM is for urgent/emergent questions only.
AK Responders Relief Line: 24/7 behavioral health for everyone working in healthcare
during the COVID-19 pandemic: 1-844-985-8275
|

