COVID-19 Alaska Clinical Update
Wednesday, October 27, 2021
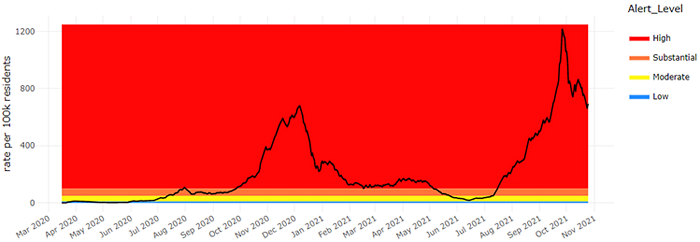
7-Day COVID-19 Case Rate – Statewide
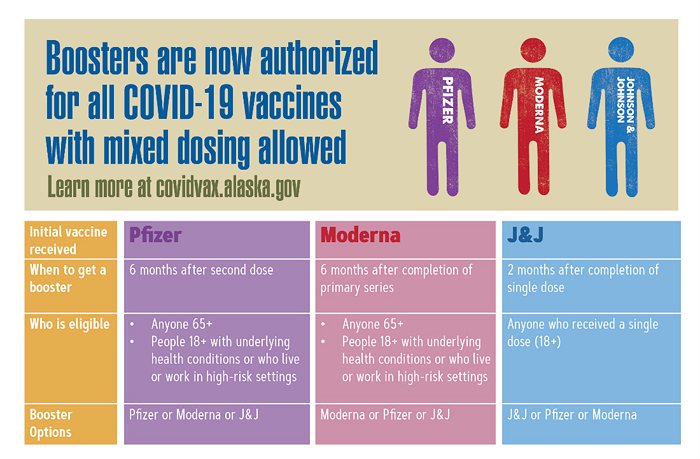
CDC recommends Moderna booster vaccine for select populations at least 6 months after their initial 2 dose series
The CDC recommends that the following groups should receive a booster shot of Moderna’s COVID-19 vaccine at least 6 months after completing their Moderna primary series (i.e., the first 2 vaccine doses):
- people aged 65 years and older
- residents aged 18 years and older in long-term care settings
- people aged 50–64 years with underlying medical conditions
CDC also recommends that the following groups may receive a booster shot of Moderna’s COVID-19 vaccine at least 6 months after completing their Moderna primary series, based on their individual benefits and risks:
- people aged 18–49 years with underlying medical conditions
- people aged 18–64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting (e.g., health care, schools, correctional facilities, homeless shelters)
CDC recommends Johnson & Johnson booster vaccine for everyone who received J&J vaccine at least 2 months after their initial immunization
The CDC recommends that everyone aged 18 years and older who received a Johnson & Johnson COVID vaccine should receive a booster dose at least 2 months after their initial immunization.
CDC allows for “mix and match” for boosters – all three authorized vaccines can be given as boosters regardless of initial vaccine brand
With the authorization of boosters for all three available COVID vaccines, on October 21, the CDC announced that eligible individuals may choose which vaccine they receive as a booster dose. Some people may prefer the vaccine type they originally received while others may choose to get a different booster. Based on data presented at the CDC’s ACIP meeting on October 21, this “mix-and-match” approach led to significantly increased levels of circulating IgG antibodies 28 days after booster vaccination. Presenters claimed that for a given primary COVID vaccine, heterologous boosts elicited similar or higher serologic responses as compared to their respective homologous booster responses”. The presented studies were not designed to show benefits in hospitalization, severe COVID illness, or death.
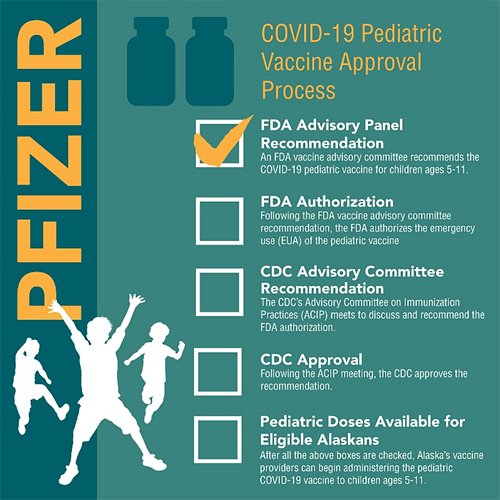
FDA’s VRBPAC recommends Pfizer-BioNTech vaccine for children aged 5 through 11 years
On October 26, the FDA’s Vaccine and Related Biological Products Advisory Committee voted to recommend amending the emergency use authorization for Pfizer-BioNTech’s mRNA COVID vaccine to allow its use in children aged 5 through 11 years. The CDC’s Advisory Committee on Immunization Practices is scheduled to meet November 2-3 to discuss the FDA’s recommendations.
Moderna announces interim results demonstrating “robust immune response” to vaccine in children age 6-11 years
Moderna submitted an application to the FDA in June to expand the Emergency Use Authorization for its mRNA COVID vaccine to children aged 12-17 years. In a press release on October 25, the company announced interim results from its Phase 2/3 trial claiming that participants in the 6- to 11-year-old range had a robust immune response to a 2-dose 50μg regimen delivered 4 weeks apart. This study enrolled 4,753 participants aged 6 through 11 years and evaluated antibody levels following vaccination as well as safety and tolerability.
*These results have not gone through peer review and were announced as a press release by the sponsoring pharmaceutical companies. The results might contain errors and report information that has not yet been accepted or endorsed in any way by the scientific or medical community.
Alaska Medical Provider ECHO – COVID Vaccination for Children 5-11 years – Information to Know
On Tuesday, November 2, from 7-8pm, there will be an Alaska Medical Provider ECHO “COVID Vaccination for Children 5-11years—Information to Know.” Pediatricians and immunology experts from around Alaska will present data on the vaccine with a focus on efficacy, dosing, and reactogenicity in children. They will also discuss how COVID has impacted other childhood vaccines and the significance of this decrease. In addition, the ECHO will address guidance for implementation and commonly asked questions providers or parents may have.
People who are moderately and severely immunocompromised may receive a fourth COVID booster dose six months after their third vaccine dose
On October 26, the CDC updated its recommendations for people who are moderately and severely immunocompromised and who completed an mRNA COVID-19 vaccine primary series. For this population, it was previously recommended that they receive a third dose of vaccine ≥28 days after the second dose. This updated recommendation now states, “A person who is moderately or severely immunocompromised and has received two doses of an mRNA vaccine and ≥28 days has elapsed since the second dose, should receive an additional mRNA dose immediately…followed ≥6 months later by a single COVID-19 vaccine booster.”
CDC updates list of underlying medical conditions associated with higher risk for severe COVID-19
The CDC recently updated its list of underlying medical conditions associated with higher risk for severe COVID-19 based on the literature available on August 31, 2021. The list of underlying medical conditions is not exhaustive and will be updated as the science evolves. CDC is currently reviewing additional underlying conditions, and some of these might have sufficient evidence to be added to the list.
No significant difference in survival without life support among patients with severe COVID-19 treated with dexamethasone 12mg versus dexamethasone 6mg
In this randomized controlled trial, 982 patients in Europe and India who were hospitalized and required at least 10 L/min of supplemental oxygen or invasive mechanical ventilation were randomized to receive either 12mg of dexamethasone or 6mg of dexamethasone for up to 10 days. The primary outcome was the number of days alive without life support (invasive mechanical ventilation, circulatory support, or kidney replacement therapy) at 28 days. The median number of days alive without life support was 22.0 days (IQR, 6.0-28.0 days) in the 12 mg of dexamethasone group and 20.5 days (IQR, 4.0-28.0 days) in the 6 mg of dexamethasone group (adjusted mean difference, 1.3 days [95% CI, 0-2.6 days]; P = .07). Mortality at 28 days was 27.1% in the 12 mg of dexamethasone group vs 32.3% in the 6 mg of dexamethasone group (adjusted relative risk, 0.86 [99% CI, 0.68-1.08]). Mortality at 90 days was 32.0% in the 12 mg of dexamethasone group vs 37.7% in the 6 mg of dexamethasone group (adjusted relative risk, 0.87 [99% CI, 0.70-1.07]). Serious adverse reactions, including septic shock and invasive fungal infections, occurred in 11.3% in the 12 mg of dexamethasone group vs 13.4% in the 6 mg of dexamethasone group (adjusted relative risk, 0.83 [99% CI, 0.54-1.29]).
CDC Morbidity and Mortality Weekly Reports (MMWR)
No increased risk of death following COVID-19 vaccine found in study of 11 million people
In this large cohort study, researchers used records for nearly 11 million persons to assess mortality not associated with COVID-19 after COVID-19 vaccination in a general population setting. Using data collected from nine healthcare organizations, this study included data from 6.4 million COVID-19 vaccinees and 4.6 million unvaccinated persons with similar characteristics as the comparison groups. To ensure comparable health care–seeking behavior among persons who received a COVID-19 vaccine and those who were unvaccinated, eligible unvaccinated persons were selected from among those who received ≥1 dose of influenza vaccine in the last 2 years. After standardizing mortality rates by age and sex, this study found that COVID-19 vaccine recipients had lower non–COVID-19 mortality than did unvaccinated persons. After adjusting for demographic characteristics and VSD site, this study found that adjusted relative risk (aRR) of non–COVID-19 mortality for the Pfizer-BioNTech vaccine was 0.41 (95% confidence interval [CI] = 0.38–0.44) after dose 1 and 0.34 (95% CI = 0.33–0.36) after dose 2. The aRRs of non–COVID-19 mortality for the Moderna vaccine were 0.34 (95% CI = 0.32–0.37) after dose 1 and 0.31 (95% CI = 0.30–0.33) after dose 2. The aRR after receipt of the Janssen vaccine was 0.54 (95% CI = 0.49–0.59). There is no increased risk for mortality among COVID-19 vaccine recipients.
Proportion of patients admitted to an ICU, required mechanical ventilation, or died did not significantly change from pre-Delta period to Delta period (July-August 2021)
In this surveillance cohort study using data from COVID-NET, researchers examined trends in severe outcomes in adults aged ≥18 years hospitalized with laboratory-confirmed COVID-19 during periods before (January–June 2021) and during (July–August 2021) Delta variant predominance. Among sampled nonpregnant hospitalized COVID-19 patients with completed medical record abstraction and a discharge disposition during the pre-Delta period, the proportion of patients who were admitted to an intensive care unit (ICU), received invasive mechanical ventilation (IMV), or died while hospitalized did not significantly change from the pre-Delta period to the Delta period. The proportion of hospitalized COVID-19 patients who were aged 18–49 years significantly increased, from 24.7% (95% confidence interval [CI] = 23.2%–26.3%) of all hospitalizations in the pre-Delta period, to 35.8% (95% CI = 32.1%–39.5%, p<0.01) during the Delta period. When examined by vaccination status, 71.8% of COVID-19–associated hospitalizations in the Delta period were in unvaccinated adults. Adults aged 18–49 years accounted for 43.6% (95% CI = 39.1%–48.2%) of all hospitalizations among unvaccinated adults during the Delta period. No difference was observed in ICU admission, receipt of IMV, or in-hospital death among nonpregnant hospitalized adults between the pre-Delta and Delta periods. However, the proportion of unvaccinated adults aged 18–49 years hospitalized with COVID-19 has increased as the Delta variant has become more predominant.
RECURRENT TOPICS
Providing COVID-19 vaccinations
In addition to the most recent CDC recommendation explained above, patients who are immunocompromised are candidates for a third vaccine dose, whether they received Pfizer-BioNTech or Moderna.
All Alaskans and people who work or live in Alaska who are aged 12 years and older are eligible for vaccination against COVID-19.
If you are interested in providing the COVID-19 vaccine in your office or clinic, please visit the COVID-19 Vaccination Program Provider Enrollment page. If you have additional questions, please email Matthew Bobo at matthew.bobo@alaska.gov
Pregnancy
On September 29, the CDC released a health advisory strongly recommending COVID-19 vaccination either before or during pregnancy because the benefits of vaccination outweigh known or potential risks.
For the latest recommendations, check out the CDC webpage on COVID in Pregnant and Recently Pregnant People and recommendations from the American College of Obstetrics and Gynecology.
Monoclonal Antibodies
Monoclonal antibody treatment for COVID-19, REGEN-COV (casirivimab and imdevimab) and Eli Lilly’s bamlanivimab and etesevimab, have been approved to treat mild-moderate COVID-19 and for post-exposure prophylaxis of COVID-19 in individuals age 12 years and older who are at high risk for progression to severe COVID-19.
If you are interested in providing monoclonal antibody therapy for COVID-19 in your office or clinic, please refer to this guide from the U.S. DHSS, and then send an email to Coleman Cutchins (coleman.cutchins@alaska.gov) and CJ Kim (cj.kim@alaska.gov) for local assistance.
For the latest recommendations, check out the CDC webpage on Monoclonal Antibodies for High-Risk COVID-19 patients and COVID-19 Monoclonal Antibody Resources for Healthcare Providers.
Ivermectin
On August 26, the CDC issued a Health Advisory about the increase in Ivermectin prescriptions and an associated rise in the number of calls to poison centers reporting overdoses or adverse effects.
A Cochrane Review published July 28 concluded, the “reliable evidence does not support the use of ivermectin for treatment or prevention of COVID‐19.” In addition, the FDA has recently created a webpage further explaining why you should not use Ivermectin to treat or prevent COVID-19 and the potential harms of taking a veterinary formulation of this mediation. Infectious Disease Society of America (IDSA) guidelines DO NOT recommend ivermectin.
Six people hospitalized in Oregon for toxic effects from Ivermectin use
In a letter to the editor published in the New England Journal of Medicine, the Oregon Poison Center reported an increasing number of calls regarding Ivermectin exposure related to Covid-19 with 21 calls in August 2021. Three persons had received prescriptions from physicians or veterinarians, and 17 had purchased veterinary formulations. Six of the 21 persons were hospitalized for toxic effects from ivermectin use; all 6 reported preventive use, including the 3 who had obtained the drug by prescription. Four received care in an intensive care unit, and none died. Of the persons who were not admitted to a hospital, most had gastrointestinal distress, dizziness, confusion, vision symptoms, or rash. Thus far, randomized, controlled trials have shown no clinical benefit in the prevention or treatment of coronavirus disease 2019 (Covid-19).
Post-acute Sequelae of COVID-19 (PASC)
15-24% of persons with COVID-19 report symptoms of cognitive dysfunction more than 6 months after initial infection
In a research letter to JAMA Open Network, researchers report data from a cross-sectional cohort study of 740 patients with COVID-19 from April 2020 through May 2021 assessing rates of cognitive impairment in survivors of COVID-19. Cognitive functioning was assessed using well-validated neuropsychological measures: Number Span forward (attention) and backward (working memory), Trail Making Test Part A and Part B (processing speed and executive functioning, respectively), phonemic and category fluency (language), and the Hopkins Verbal Learning Test–Revised (memory encoding, recall, and recognition). The mean age of 740 participants was 49 years, 63% were women, and the mean (SD) time from COVID-19 diagnosis was 7.6 (2.7) months. The most prominent deficits were in processing speed (18%, n = 133), executive functioning (16%, n = 118), phonemic fluency (15%, n = 111) and category fluency (20%, n = 148), memory encoding (24%, n = 178), and memory recall (23%, n = 170). In adjusted analyses, hospitalized patients were more likely to have impairments in attention (odds ratio [OR]: 2.8; 95% CI: 1.3-5.9), executive functioning (OR: 1.8; 95% CI: 1.0-3.4), category fluency (OR: 3.0; 95% CI: 1.7-5.2), memory encoding (OR: 2.3; 95% CI: 1.3-4.1), and memory recall (OR: 2.2; 95% CI: 1.3-3.8) than those in the outpatient group. Patients treated in the ED were more likely to have impaired category fluency (OR: 1.8; 95% CI: 1.1-3.1) and memory encoding (OR: 1.7; 95% CI: 1.0-3.0) than those treated in the outpatient setting. Impairments in executive functioning, processing speed, category fluency, memory encoding, and recall were predominant among hospitalized patients. The relative sparing of memory recognition in the context of impaired encoding and recall suggests an executive pattern.
For the latest recommendations, check out the CDC webpage on Post-COVID-19 Syndrome and Evaluating and Caring for Patients with Post-COVID conditions
Myocarditis
For the latest recommendations, check out the CDC webpage on myocarditis and COVID-19 vaccines
COVID-19 Speakers’ Bureau
Anyone can request a free presentation for a group interested in learning more about the COVID-19 vaccines available in Alaska.
Aside from COVID-19
CDC and ACIP release recommendations for seasonal Influenza vaccination
Routine annual influenza vaccination is recommended for all persons aged ≥6 months who do not have contraindications. Influenza vaccine may be administered at the same time as COVID-19 vaccine. Detailed recommendations for influenza vaccination for persons currently infected with COVID-19 are available from CDC.
Upcoming Events/Conferences/Presentations
ANTHC Tribal Health Webinar Series
The ANTHC Tribal Health Webinar series occurs on Friday from 12-1pm on Zoom and is open to the public. Here is the upcoming schedule for the fall and the Zoom link.
11/05: Rosalyn Singleton, MD: Respiratory/RSV/COVID Hospitalization trends and future interventions.
11/15: Mary Owen, MD: Tlingit People
11/19: Katie Presser, PharmD: Statewide Antimicrobial Stewardship
12/03: Marah Gotcsik, MD: ANMC Guideline on Preterm Infant Nutrition through 2 Years Old
12/10: Leslie Kerzner, MD: Care of the NICU Grad for Primary Care Providers
Join Zoom Meeting
https://anthc.zoom.us/j/98667611681
Meeting ID: 986 6761 1681
One tap mobile
+16699006833,,98667611681#
Use of Valid Background Check Clearances by Multiple Employers
Providers who have applicants with pending background checks with DHSS BCU may allow individuals to start work prior to the Background Check Program completing their check IF the applicant has documented proof of having a current Alaska DHSS background check (provisional or complete) for another DHSS provider. The applicant must provide their new employer a copy of the final background check eligibility letter for the other provider, and providers are required to maintain a copy of that eligibly document in the employee’s file. Providers who hire employees in this manner MUST provide supervised access to those employees, i.e., to ensure the protection of recipients of services, the provider must maintain a prudent level of awareness of the whereabouts of an individual for whom supervised access is required. Employees working in this way may NOT be the only individual working in a facility or a setting, as another employee must be present to provide the supervised access. The provider’s oversight agency will monitor providers to ensure they are in compliance with these requirements, and providers must submit proof of compliance to those agencies upon request. Questions? Please contact your DHSS oversight division.
CDC Clinical Support: There is a Clinician On-Call Center, a 24-hour hotline with trained CDC clinicians standing by to answer COVID-19 questions. Call 1-800-CDC-INFO (800-232-4636) and ask for the Clinician On-Call Center.
The most up-to-date, evidence based COVID-19 treatment guidelines can be found at:
IDSA Guidelines on the Treatment and Management of Patient with COVID-19
NIH COVID-19 Treatment Guidelines
Alaska Responders Relief Line (844) 985-8275
Your well-being matters. Your behavioral health colleagues are standing by to talk 24/7: 844-985-8275
Recognizing the unique stressors that providers face, the Division of Behavioral Health has established a 24/7 support line, (844) 985-8275, for healthcare and behavioral professionals impacted by COVID personally and professionally. Staff supporting the call line recognize callers are often first responders and will allow callers to openly express their experiences and feelings serving Alaskans impacted by COVID.
This service is also available to immediate family members of first responders who may be experiencing stress, anxiety and other hard to label emotions as a result of their loved one engaging on the front lines.
AK Clinical Reminders — UPDATED October 27, 2021
COVID-19 testing guidelines and test site locator

These ECHO sessions are produced and facilitated by
UAA’s Center for Human Development Alaska ECHO project
in partnership with the State of Alaska, Department of Health & Social Services
Session information and recordings of previous ECHO sessions
subscribe to ECHO calendar updates | email: echo@alaskachd.org | website: akecho.org
Upcoming Session Highlights:
Pop-Up ECHO: Training for Pediatric Vaccine Administration
This Friday, Oct. 29th from 12-1pm
Registration link: https://echo.zoom.us/meeting/register/tJMsf-Ghrz8jG9z6nOsEIMtUs1qLyB4wlasC
This special pop-up ECHO session aims to support Vaccine Providers in advance of the anticipated approval of the COVID-19 vaccine for ages 5-11. This session will offer demonstrations of techniques, share what resources for providers are available, COVID-19 updates, and provide time for Q&A discussion with our hub team of experts.
Palliative Care ECHO
Tuesday Nov. 2nd from noon-1pm
Registration link: https://echo.zoom.us/meeting/register/tJIrcO2gqTksGtztVm5GiISIXI7vMidLpWBO
Our next session will include a didactic presentation Meeting People Where They Are: Providing Palliative Care to Rural Populations by guest presenter Nancy Joiner APRN, ACHPN from the University of North Dakota’s Center for Rural Health, and end with an open forum where providers can share their knowledge and experience, and participate in a Q&A session with our hub team of experts.
Regular Series
**Join us for 2 new and returning ECHO series on Behavioral Health & Addictions, starting November 2021**
Co-Occurring Behavioral Health, Opioid and Stimulant Use Disorders ECHO Returning with new didactics!
1st & 3rd Wednesdays from 12:00pm-1:00pm, November 3, 2021 - April 20, 2022
The Co-Occurring Behavioral Health (COBH), Opioid and Stimulant Use Disorders ECHO facilitates a virtual network for behavioral health providers to learn best practice care through real-time access to experienced subject matter experts and their peers. Each session includes a brief lecture, de-identified case presentation for participants to receive feedback on complex cases, and open discussion facilitated by an interdisciplinary team.
Data Waivers ECHO New ECHO!
2nd Wednesdays from 12:00pm-1:00pm, November 10, 2021 - September 14, 2022
The Data Waivers ECHO facilitates a virtual network for clinical providers to learn and implement best practices for offering buprenorphine and other medically assisted treatment (MAT) services under a data waiver. Each session includes a brief lecture, de-identified case presentation for participants to receive feedback on complex cases, and open discussion facilitated by an interdisciplinary team.
Alaska Medical Provider ECHO (formerly COVID-19 for AK Healthcare Providers)
Bi-monthly on the 1st and 3rd Tuesday of the month from 7-8 pm
This ECHO aims to increase knowledge and share best practices among medical providers across Alaska as well as to increase access to information for those living in rural areas of the state.
School Health ECHO
Every Monday from 3:30-4:30 p.m Register
The School Health ECHO is a virtual learning network intended for professionals in the education setting (administrators, school-based nurses, etc.) to interface with a team of medical and education experts in Alaska.
Vaccine ECHO for Providers
Weekly on Tuesday from 2-3 p.m. Register
The Vaccine ECHO for providers provides planning and operation updates to vaccine providers across Alaska, while answering any questions you may have.
Palliative Care ECHO
Monthly on the first Tuesday from 12-1 p.m.
This monthly ECHO is for all Alaskan healthcare disciplines supporting patients with serious illness, and aims to provide support and up-to-date information regarding Palliative Care during this period of COVID-19.
Public Science ECHO
Weekly on Wednesday from 12-1 p.m. register via Zoom
The Alaska Public Health Science ECHO is a virtual learning network intended for the general public to interface with our Public Health Leadership Team to explore the science of the COVID-19 virus, other public health topics, and current best practices. Or view via concurrent livestream to Facebook: https://www.facebook.com/akechoprograms
Local Government Public Health ECHO
Monthly on the third Wednesday from 3-4 p.m. Register
The Local Government Public Health Analysis ECHO is a virtual learning environment intended for local Alaska government leaders to interact with the State Public Health Leadership team and focuses on pandemic mitigation tools available, and how to use them.
Long Term Care Facilities ECHO
Second Wednesday of the month from 4-5 p.m. Register
Please join other staff and administrators of Alaska’s assisted living homes and residential care facilities to gather, learn, share, and grow. COVID has disrupted the fabric of our daily life and we can always learn from each other as we adjust to the new normal.
Healthcare Specific Situational Awareness ECHO
Weekly on Thursday from 12-1 p.m. Register
The Healthcare Specific Situational ECHO is a virtual learning network intended for healthcare professionals to interface with our Public Health Leadership Team to explore current best practices and the most recent information related to Public Health.
Perinatal ECHO
Monthly on 3rd Thursday from 6-7 p.m. Register
The Alaska Perinatal ECHO is a virtual learning network intended for medical providers caring for pregnant patients and their newborns.
EMS ECHO
Monthly on the 1st and 3rd Wednesday 1-2 p.m Register
The EMS ECHO is a virtual learning network intended for Emergency Medical Services and related personnel in Alaska to amplify best practices. Sessions are topic-driven and typically include a guest presenter or a brief lecture with an interactive case or process discussion.
AK COVID-19 clinical hotline for physicians: 833-751-4212. Staffed 24/7.
8PM-8AM is for urgent/emergent questions only.
AK Responders Relief Line: 24/7 behavioral health for everyone working in healthcare
during the COVID-19 pandemic: 1-844-985-8275
|
|
