 Since its launch, Hennepin
Health staff and members have consistently identified lack of housing as a top
health barrier. Consequently, housing homeless or precariously
housed members is a priority.
When care coordination teams
identify a medically complex or frequently-hospitalized member who is
experiencing homelessness or is precariously housed, they make a referral to
Hennepin Health’s Social Service Navigation Team. Through relationships with
community-based housing providers, the navigators assess each member’s
situation and match them to available supportive housing options.
In June 2015, Hennepin Health’s
data analyst looked at 123 members who were housed by Hennepin Health’s
Social Service Navigation Team between 2012 and mid-2014 — and analyzed their rates
of emergency department (ED), psychiatric emergency department (APS), and inpatient
hospital admissions, and outpatient clinic visits one year prior to and one
year following their housing placement.
Evaluation methodology
- Utilization rates
are reported on a per 1000 member month basis, and the pre- and post-periods
are each 12 months in duration
- All outcomes are
calculated from electronic health record (EHR) data
Results
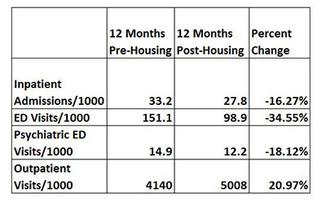 Hennepin Health members housed through housing navigation
services saw significant reductions in acute care utilization following
placement.
- Members were admitted to a hospital 16% less often after placement in housing
- Members visited the emergency department 35% less often after placement in housing
- Members visited the psychiatric emergency department 18% less often after placement in housing
- Members received outpatient clinic visits (including primary care) 21% more often after placement in housing
Back to top
 On June 15, Hennepin Health and Hennepin County
Medical Center were honored to host colleagues from
the New
Jersey Health Care Quality Institute, Centrahealth, Virginia Commonwealth University, New York University School of Medicine, National
Opinion Research Center at the University of Chicago and the American Board
of Family Medicine.
Attendees
enjoyed a morning of presentation and discussion with a variety of Hennepin
Health team members, followed by a tour of Hennepin
County Medical Center’s Coordinated Care Center (CCC) and Hennepin Health Access Clinic — and
observation of an inter-disciplinary team meeting.
Many of the
participants were visiting Minneapolis for the 2015 AcademyHealth
Annual Research Meeting (ARM) – the nation’s largest health services research conference. Hennepin
Health was represented at this meeting in two panel presentations on community
health and accountable care, serving as a model that others are interested in
replicating nationally.
Back to top
 In May 2015, Renee Levesque became Hennepin Health’s Social Service
Navigation Team supervisor. Renee comes from Touchstone Mental Health, where she
served as the director of Targeted Case Management and Intensive Community
Rehabilitation Services. Renee’s worked on multidisciplinary teams and with
vulnerable populations — two Hennepin Health mainstays — her whole career.
Renee is attracted to Hennepin Health’s innovation, and the program’s
long-term, holistic approach to health. A self-described “fiscal conservative”
she also admires Hennepin Health’s attempts to reduce unnecessary health care
expenditures — while increasing client health and well-being.
Renee will focus on building more efficiency into Hennepin Health
processes.
One of Renee’s revelations from working in the human service field is
that everyone is complex and “relevant.” “You see people [as they are] in that
moment,” she said. “But I’ve learned that if you listen to people with empathy
you find that everyone has a story, everyone comes from some place, and
everyone has dreams, feelings, and goals that they want to achieve.”
You can contact her at Renee.Levesque@hennepin.us
Back to top
Trauma Informed Care (TIC) is the belief that a quality health care, human
services and/or social safety net organization needs to address the impact of
trauma on every person in that organization. Hennepin Health supports trauma informed care and is committed to working with its clinics and providers
to implement TIC principles.
For the past
few months, each issue of the Hennepin Health newsletter has featured one of
the seven TIC domains. We share practical ways to implement that domain and
showcase examples of current work that supports it. This issue focuses on
Domain #3.
Domain
#3: Nurturing a trauma informed and responsive workforce, Part Two -- Recognizing
the impact of secondary trauma on caregivers.
We can’t practice trauma informed care without addressing the impact of
trauma on ourselves. Working in a caregiving environment comes with an
emotional cost that can lead to personal and professional consequences. This
installment will address the impact of secondary trauma — and offer coping strategies.
To begin: What is the emotional cost of caring for clients and
patients?
Burnout, compassion fatigue, secondary trauma and vicarious trauma are all terms that describe the impact of working in a caregiving environment. Ironically, those
who bring the most empathy and passion to their work are often the most at risk
— because when we put our whole selves into work, it can be difficult to find a
balance between helping others and caring for ourselves.
Laura van Dernoot Lipsky, founder
and director of the Trauma Stewardship Institute and author of Trauma Stewardship: An Everyday Guide to
Caring for Self While Caring for Others, calls the concept of caring for people who are suffering “trauma
stewardship.” Her book is a great resource as is her TED talk on the subject.
 We can use the following steps to assess our vulnerability to secondary
trauma, determine the impact of our work, and make positive changes in our lives:
1. Understand
and accept our vulnerability.
The first step is
simple: awareness. Knowing that we are vulnerable to being impacted by our work
can go a long way towards prevention. If we aren’t aware of this, the symptoms
below may be scary and cause us to intervene in ways that don’t address the root
of our distress.
2. Understand the symptoms. Individuals impacted by
caregiving work may experience:
- Emotional: stress, anxiety, numbness
- Intrusive cognitions: thoughts, images,
nightmares, dreams
- Perceptual cognitions: altered worldview, memory
loss, loss of interest, jaded
- Physiological: depression, headaches, digestive
problems, low energy
- Behavioral: being tearful, over-reactive, numb,
forgetful, sleepy, nervous, excessive substance use, withdraw socially,
judgmental, unsympathetic
- Interpersonal: codependency, isolation from
others, loss of trust, loss of interest in sex, loss of intimacy, blaming
others, family problems
Check out this professional
quality of life inventory online.
3. Understand preventative and reactive coping
strategies.
Achieve balance:
- Learn to balance the needs of our clients,
agency and self: Pressures resulting from work frequently compete with the time
we have to take care of ourselves. Often we choose work. Do this too much and
we will lose balance and effectiveness in all areas.
- Recognize when our self-care system is not
working: Most of us can list sources of self-care, but are we really utilizing
them? And do they really work for us?
- Recognize our own positive and negative coping
behaviors: Understanding what helps and hurts is an important first step
towards creating a self-care plan that works.
- Commitment to personal replenishment: This is
hard, but crucial. We need to be replenished. The activities that accomplish
this may feel indulgent and selfish, but that’s how we know they’re working.
Make changes to how we work:
- Avoid grouping emotionally stressful tasks
together: Think about the tasks we put off doing. The energy we put into that
avoidance stays with us throughout the day and distracts us from the good
things. Do those tasks throughout the day or week, proactively, and we’ll feel
much better.
- Plan breaks throughout the workday and follow
through: When we are able to take a break, TAKE A BREAK. Walk outside for fresh
air, take a couple of deep breaths.
- Stretch throughout the day to reduce tension
build-up.
- Answer “let me think about this” rather than
automatically accepting new tasks.
- Take professional development and training
opportunities: Stepping away to learn new information will increase our
motivation and camaraderie with others.
- Get involved with our community in another area
of the field or a related cause: For example, if we work with children who are
sick or dying it can be easy to forget that many survive and are healthy and
happy. Attend a survivor’s event or walk to experience this.
4. Get help: Employee Assistance Programs
The July newsletter’s trauma informed care installment will
focus on management and organizational strategies.
Back to top
This is part two of a two-part series
Lafonso Rollins. Read
part 1 here.
Part
2: Post-Prison
On July 12, 2004, in an Illinois
courtroom, a judge exonerated 28-year-old Lafonso Rollins of raping a 78-year-old woman.
Rollins had been charged with the rape in January 1993 — and he served
4,193 days of a 75-year prison sentence. He might have been in prison even
longer had it not been for "Bull," a fellow inmate who helped Rollins draft a
post-conviction relief petition and a motion for DNA testing.
Ultimately Rollins was assigned a
public defender and obtained DNA test results — which were not made available during his original trial.
The results excluded Rollins as the perpetrator of the sexual assault. He was
released from prison in July 2004.
John Gorman, a spokesman for the Cook County
State’s Attorney's office told
the Chicago Tribune that after the judge read the not guilty verdict, “It was one of the
only times I have seen a public defender and prosecutor hug each other.”
Minutes after that hug, Rollins left
the courtroom. But the moment was bittersweet. Rollins had nowhere to go and no
one to greet him, because most of his relatives had died shortly
before, or while, he was in prison.
In
early 2006, Rollins filed a lawsuit against the City of Chicago. The suit alleged that Rollins
falsely confessed to the rape because city police detectives used “excessive force, intimidation,
threats and misrepresentations.”
Rollins eventually agreed to a settlement after his defense
discovered documents that revealed the Chicago Police Crime Laboratory had
improperly handled his case.
***
After the settlement, Rollins purchased a condo near West Madison Street and North Oakley
Boulevard. But he soon encountered other “prisons.”
One of these prisons, said
Rollins, was his “institutionalized mentality.” He wishes he’d used his
settlement money to “travel the world”; instead he holed up inside his condo.
It took him a year after he was released to feel comfortable outdoors.
Rollins’ family was another thing he had to contend with. Shortly after
his release, Rollins went to visit his younger sister. He was horrified
when he saw her neck. She’d been stabbed with glass, and had over 150 stitches.
“These are the impacts of my life,” he said of that image, which won’t go
away. “These are my demons.”
Ironically, Rollins’ newfound wealth was the biggest prison. Many
“friends” wanted his settlement money, and he was hounded incessantly. People
even “stormed” his condo.
When Rollins’ mentor advised him
to leave Chicago, he moved to Georgia. And, according to him, “From there, I
got lost.”
***
“I regret losing myself,” Rollins says now, of the next eight years,
during which time he lived in Georgia, Florida, Illinois, and Minnesota. “I
learned that money can’t solve everything.”
While Rollins made charitable donations
to the Innocence Project (an organization that helps exonerate wrongfully
convicted individuals) and to Chicago’s Pilgrim Baptist Church (which had been
devastated by a 2006 fire) other money was squandered. It went to things that ultimately
made him anxious and alienated.
In Georgia, “I spent my time in a Best
Buy parking lot,” Rollins recalled, “because it was a place where no one would
expect me to be. Everything was negative.”
Recently, Rollins relocated to
Minnesota, where he’s struggled with substance abuse and anxiety. A few months ago, he joined Hennepin Health.
***
In 2015, Hennepin Health
strengthened its relationship with chemical dependency and mental health
treatment facilities like Park Avenue Center, RS Eden, NuWay,
and Anchor House.
Some of these facilities are now — with member
permission — sending Hennepin Health the names of people who are in the
facilities and due to transition out. After receiving these referrals, Hennepin
Health social service navigators reach out to the members in advance of their
transition.
DeAnna
Hayden, a Hennepin Health social service navigator, explains the goal: “If we
can catch people before they’re actually discharged we can try to meet some of
their social service needs so that when they get discharged they don’t end up,
say, back in the shelter — or get out and don’t have anything lined up in terms
of follow-up care.”
Hayden
connected to Rollins through this transition process. She helped him obtain a chemical
dependency assessment and get into an outpatient treatment program. She also
helped place Rollins in a studio apartment that Hennepin Health leases from the
Minneapolis Public Housing Authority.
Today,
Rollins participates in Hennepin Health’s ED In Reach program, a collaboration
with RESOURCE Chemical and Mental
Health. Holly Sandefer, the RESOURCE social worker who
facilitates the program, provides targeted case management to Hennepin Health
members who are frequent users of the emergency room and other crisis care.
Rollins
visited the emergency department four times in the two months before he started
working with Sandefer. Since joining ED In Reach, he’s only been to the
emergency department once; since being housed he has not visited the emergency
department at all.
***
On
May 20, Hayden and Sandefer visited Rollins at his apartment.
That day, Rollins told Hayden and Sandefer that he
desires more social connections and would like to be a motivational speaker. He
wants to “get involved,” “to be part of something,” but he isn’t sure how to
take the next step. He shared stories from his life, revealing a penchant for
spoken word poetry, and questioned whether his past experiences can take him
from Point A to Point B.
“You’ve learned phenomenal life lessons that
some people never get in their whole life,” Sandefer assured him. “You have a
voice that’s really important for other people to hear.”
Added Hayden, “The person you are and the
attitude you have is astounding.”
If you know of motivational speaking opportunities
for Rollins, email DeAnna.Hayden@hennepin.us
Back to top
|

